Managing congestive heart failure in a Medicare risk popula
advertisement

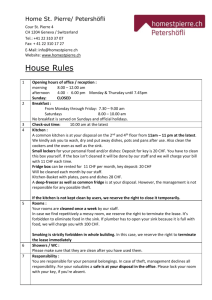
Managing CongestiveHeart Failure in the Medicare Risk Population The health issues a of our growing population of elderly patients present challenge and an opportunity to improve care. Recent changes in the Health Care Financing Administration's Medicare program have opened new opportunities for managed care organizations (MCOs). In fact, the Medicare Risk Program may be one of the last remaining frontiers for many MCOs. Any new population presents a range of challenges. Wellpoint Pharmacy Management, a pharmacy benefits manager (PBM) responsible for 15 million lives, prepared itself to deal with a geriatric population's existing health problems and futures William]. Waugh, Pharm.D. filled with increasing illness by seeking out possible models in existing programs. Wellpoint's approach applied the traditional principles of managed care to this new group of members. An executive team of pharmacists and physicians reviewed statistics about the elderly in general, and Disease State Management and Outcomes Research, Wellpoint Pharmacy Management, Calabasas Hills, CA AUTHOR CORRESPONDENCE: William}. Waugh, Pharm.D., DirectOl; Disease State Management and Outcomes Research. Wellpoint Pharmacy Management, 2700.1 Agoum Road, #325, Ca/abasas Hills, CA 91361 CopylightlJ) 1999, Academy oj Managed Care Pharmacy, Ine. All rightsreserved. 14 Journal of Managed Care Pharmacy ]MCP interventions: impaired quality of life, and the occurrence of atrial fibril1ation in approximately 50% of patients, a complication that can drain health care dollars. Expenditures for treatment of CHF in the U.S. exceed $10 billion annually (see Figure 1). Hospitalization accounts for about $7 billion, and rehospitalization is a serious concern. Long-term care facilities and physician's office visits consume ment for congestive heart failure (CHF) and screening for inappropriate or unne- especially in reducing hospitalizations."} Savings potential is even greater when cessary drug use. population trends are considered. As the likelihood of developing CHF increases Medicare risk population revealed that CHF is the most common DRG reported, is Director, prevalence of CHF doubles with each decade. Two complications of CHF are ideal targets for managed care program savings could be realized: disease manage- The need f<?rthis plan was based on two significant findings: 1) analysis of diagnosis-related groups (DRGs) in the WILLIAM}. WAUGH, PHARMD, years after diagnosis. After age 50, the about 20% of the total! Though drugs, at $230 million annually, represent only about 2.3% of total expenditures, drug treatment employed properly and aggressively could reap significant savings, the Medicare Risk group in particular, and identified two areas where considerable Aut/u}/ The Framingham Study found that the mortality rate for CHF is high; only 38% of men and 57% of women survive five with age (see Figure 2), unless prevention is emphasized and optimal drug therapy is prescribed consistently, cases of CHF can only increase as our population and 2) data on hospital admissions related to adverse drug reaction in the elderly, along with information collected by the ages.4 National Medical Expenditure (NME) Survey of 1987, showed that inappropriate' drug use remains a problem in the elderly. clini,cal guidelines for treatment of CHF that have been applauded by specialists.l CONGESTIVE HEART FAILURE The Agency for Health Care Policy and Research (AHCPR) has published Approximately 18 months ago, Wellpoint developed a disease management program based on these guidelines and sev- CHF affects more than 2 million Amer- eral clinical studies. Treatment guidelines also were established for atrial fib- icans, with 400,000 new cases diagnosed annually. It is twice as prevalent in men. rillation because of its high incidence and cost, and the excellent response of January/Febru"ry 1999 Vol. 5. No.1 Managing Congestive Heart Failure in the Medicare Risk Population Figure 1. Total Direct Expenditures for CHF in the United States patient outliers are identified to determine Total Direct Cost: $10 billion annually (in millions of dollars) where interventions can make the most impact. Improvement begins with educa- . . . Hospital Drug ting patients; intensive patient education includes case management. Case managers, all nurses, call patients at least monthly-more often if the patient is high risk. They prompt Nursing Home Physician Office Visits $1,900 patients when medication refills are due, remind them that daily weighing can help detect fluid retention and its complications, and educate patients on symptoms that should be reported to their physicians. Whenever contact is made, the case manager sends documentation to the physician by fax or mail. Case managers track standard outcome measures, including frequency of office visits, use Clearly, use of these drugs is people with CHF to drug therapy. The goals were to improve quality of life, reduce admissions and readmissions related to decompensation, and shorten length a This program was applied to a group of state employees in a southeastern state during its first six months of operation. Though its full impact after 18 tice. Each plan that adopts our program is allowed to modify treatment guidelines of stay The steps used to identify patients included risk assessment based on pre- to meet the concerns of its own advisory panel of cardiologists and internists. All plans reviewed the gUidelines; more than 90% accepted them as written. The re- scription records and presence of an ICD-9 code for CHF if hospitalization had occurred; demographic modeling mainder made small modifications based on specific demographics of their mem- by age, gender, and address; and indivi- bers. Concerns raised dual patient identification. The treatment guidelines were simple but thorough, increased bleeding risk as the average age of the population rises, and the popula- emphasizing appropriate drug use. The best practices identified were the use of angiotensin converting enzyme (ACE) tion's ability to tolerate ACE inhibitors. months has not yet been measured, we predict a decrease in hospitalizations of up to 40% within the first year. DRUGS CONTRAINDICATED IN THE ELDERLY by some include Despite years of information dissemination by various agencies, the problem of unnecessary drug use in the elderly still exists. Our research revealed that of Some plans discussed other, more basic concerns such as cost and dosing regimen. inhibitors in all CHF patients to decrease mortality and the use of low-intensity Pharmacy and medical claims are ana- NME Survey's list of 20 drugs inapelderly (see Table 1) the for propriate being still used with alarmmany were the lyzed every six months to identify opportunities for improvement. Prescriber and warfarin (international normalized ratio [INR] between 2 and 3) in most atrial Figure 2. Prevalence of Heart Failure by Age fibrillation patients to decrease incidence of stroke. Employing a best-practice model ensures quality care and promotes physician 10 8 buy-in. Although firm research supports the use of both ACE inhibitors and warfarin in CHF patients, use of these agents has not increased appreciably in the last ~ five years.s As we began the disease ~ management program, both drugs were used by less than 40% of our patients. More-over, about 20% of our prescribers did not employ the INR to monitor warfarin, even though the INR is the of ACE inhibitors, complications, and number of hospitalizations. best prac- _I.&.1988-911 . .. 1976-80 6 OJ .. u .... OJ 4 .. . . 0 ~ . .. 2 30 35 40 45 . . 50 55 60 65 70 75 80 Age best indicator of its therapeutic efficacy ( VoL 5, No. 1 January/February 1999 jMCP Journal of Managed Care Pharmacy 15 Managing Congestive Heart Failure in the Medicare Risk Population Table 1. Contraindicated Drugs in the Elderly Suggested Alternative(s) Drug Name Reason diazepam daytime sedation, risk of falls - temazepam, estazolam chlordiazepoxide daytime sedation, risk of falls temazepam, estazolam f1urazepam daytime sedation, risk of falls temazepam, estazolam meprobamate daytime sedation, risk of falls temazeDam, estazolam pentobarbital daytime sedation, risk of falls temazepam, estazolam secobarbital daytime sedation, risk of falls temazepam, estazolam amitriptyline anticholinergic effects, risk of nortriptyline, desipramine orthostatic hypotension indomethacin risk of CNS toxicity other NSAIDs chlorpropamide risk of SIADH syndrome other hypoglycemics propoxyphene risk of CNS & cardiac toxicity acetamin9phen pentazocine risk of CNS & cardiac toxicity acetaminophen isoxsuprine no demonstrated efficacy cyclandelate no demonstrated efficacy dipyridamole headaches and dizziness aspirin cyclobenzaprine risk of CNS toxicity acetaminophen methocarbamol risk of CNS toxicity acetaminophen orphenadrine . risk of CNS toxicity trimethobenzamide no demonstrated efficacy, risk of drowsiness, diarrhea other antiemetics propranolol risk of CNS toxicity atenolol, nadolol methyldopa risk of CNS toxicitv atenolol, nadolol reserpine risk of CNS toxicity atenolol, nadolo] guanethidine risk of hypotensive episodes ateno]ol, nadolol guanadrel risk of hypotensive episodes ateno]ol, nadolol ing frequency in some areas.6 These drugs can contribute to falls, impair cognition, or cause other distressing adverse ing the particular agent of concern, and asking for consideration of an alternative agent. Three months after the letter was effects. sent, we reviewed each case. Another let- Figure 3 describes our program. In a three-month baseline study, we identified patients for whom one or more of these drugs was prescribed, first approaching pre- ter then was sent to either thank the physician for cooperating or, if necessary, again suggest an alternative. At a plan in the northeast, of the first 500 Medicare Risk patients who enrolled, 15% were taking a contraindicated drug. scribers rather than patients. Prescribers received a plan-approved letter describ- of patients. In most cases, the problematic drug was disco"ntinued. Outcomes are not easy to measure in this project. It is difficult to determine how much quality of life improves, or how many hospitalizations or falls are prevented. We are working, however, to find a way to determine indirect costs and specific patient outcomes. CONCLUSION The programs described here were designed for the aging populations in our plans; their successes can be applied to Medicare Risk members as enrollment risk of CNS toxicity carisoprodol After intervention, changes in drug therapy were made for approximately 70% increases. In CHF disease management, appropriate and aggressive use of drugs is an effective way to decrease other costs. Enhancing the program with case man- agement services is an important way to ensure quality care to this fragile population. Reviewing claims for unnecessary or contraindicated drugs and taking action with prescribers alleviates the risk of adverse events. We plan to expand our contraindicateddrugs program by integrating our data with medical information, looking for patient-specific outcomes, examining comorbidities, and using innovative medical resources. These measures will be incorporated to help quality improvement programs acquire or maintain National Committee for Quality Assurance accreditation, and will be reflected in HEDlS and other performance measures. .... References Konstam M, Dracup K, Baker D, et aL Heart with leftventricular dysfunction. Clinical Practice Guideline 1. faiJure: evaluation and care of patients Figure 3. Program Flow Plan Approval of Pre-study ~ 3 Months 16 Letter Follow-up 3 Months Follow-up 3 Months UU Mail Mail Letters Letters Journal of Managed Care Pharmacy jMCP JanuarylFebruary 1999 Final Analysis 1'Morith u No. 11, AHCPR Publication No. 94-0612. 2. Vinson JM, Rich M\V, Shah AS, et aL Early readmission of elderly residents with congestive heart faiJure. JAm Geriatric Soc. 1990; 38: 1290-95. HM, Parent EM, Tu N, et aL Readmission after hospitalization among Medicare beneficiaries. Arch Intern Med 1997; 157: 99-104. 3. Krumholz 4. National Health and Nutrition Examination Survey (1976-80 and 1988-91), National Center for Health Statistics. 5. Stafford RS. Use of ACEI's in CHI' Arch Intern Med; 157: 2460-64. Vol. 5, No.1