Lab Exer 7 Urinalysis
advertisement

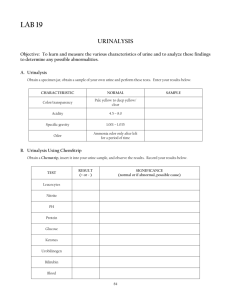
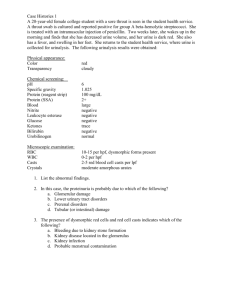
Laboratory Exercise 7: Urinalysis Urine is a solution of the solvent water in which there are dissolved salts and N-waste products (NPNcompounds) urobilinogen from bilirubin, urea from protein metabolism, uric acid from nucleic acid metabolism and creatinine from muscle metabolism. Urine is produced when blood plasma is filtered and secreted by the kidneys. Eating, drinking and physical activity cause changes in urine composition and volume. Analyses of random samples collected at different times of day show wide variations. Samples taken over 24 hours reflect accurately the kidney function. Random samples are used for routine analysis. Change in urine composition can indicate a disruption in homeostasis. Urinalysis includes physical, chemical and microscopic examination of the urine is a routine procedure that provides clinically significant information. Physical Tests 1. Volume – Normal value 1500 mL/24 hr (about 1 m1/min.) 2. Specific Gravity (SG) – indicates total solute concentration in the urine by comparing concentration of solute in the urine to that of pure distilled water. SG is derived by comparing the density of urine to the density of pure distilled water (1.000 g/mL). If an unknown sample (in g/mL) were divided by 1.000 g/mL, a specific gravity index would be obtained. Normal specific gravity values 1.0081.030. SG measures the kidneys concentrating or diluting ability of the filtrate formed as it passes through the kidney nephrons. A SG of 1.010 for urine indicates it has the same density as protein-free plasma. As the filtrate passes through the nephrons it becomes concentrated and the urine SG rises above 1.010. SG values vary in normal individuals considerably, reflecting variations in fluid and solute intake and loss. SG values are clinically significant. SG provides information regarding the state of hydration of the individual; highly concentrated urine implies dehydration. In progressive kidney disease, the SG range gradually narrows to become fixed at 1.010 at this value the nephron’s reabsorptive capacity is non-functional as the urine SG is the same as the SG as protein-free plasma. Refractometer method of determining SG – is based on the theory that molecules in solution refract or bend light waves. The degree of refraction is proportional to the concentration of the solute (density or SG) in a solution. 3. Color – Freshly voided urine is pale to dark yellow. The color is due to the catabolism of hemoglobin. hemoglobin (red) → hematin → bilirubin → urobilinogen 1 → urochrome and urobilin (yellow) The concentration of solutes influences color intensity. The more concentrated the urine solute, the less water, the darker its color. The darkness of the morning urine, indicates its relatively high SG due to overnight water reabsorption. 4. Turbidity - Freshly voided urine is normally clear and transparent. On standing urine becomes cloudy or turbid, due to precipitation of solute (such as phosphate and urate salts) out of solution. Turbidity on initial voiding may indicate blood proteins that filtered in the urine, mucus, pus or a large number of bacteria. Chemical Tests 5. Protein, Glucose, Hemoglobin, Bilirubin and pH a. Protein in the urine – albuminuria. Albuminuria can occur in a normal kidney after strenuous exercise. b. Glucose uptake impaired by body cells, the glucose concentration rises in the blood, hyperglycemia. When the renal tubule reabsorption capacity for glucose is exceeded glucose appears in the urine, glucosuria. c. Hemoglobin in the urine – hemoglobinuria. Hemoglobin is released from the red cells by hemolysis either in the blood or within the urinary tract. d. Bilirubin appears in the urine normally in very small amounts as a hemoglobin breakdown product. It’s further conversion to urochrome gives the yellow color to the urine. Large amounts of bilirubin in the urine, bilirubinuria, is caused by liver infection or toxicity. f. pH of the urine reflects the kidney’s ability to maintain body fluids neutral (pH 7.4). Vegetarian diets yield an alkaline pH, while eating a normal mixed diet promotes the formation of weak acids and a urinary pH 5-7 (avg.6.0). 6. Ketones - The presence of glucose and ketones in the urine can help diagnose diabetes. When glucose is not properly used as an energy source, the body uses fat. Ketones are the by-products of fat oxidation. Normally, all ketones are metabolized to CO2 and H2O and none are excreted. In diabetes, the abnormal blood level of the ketones spillover into the urine. Normal Values Protein none to trace Glucose none to trace Hemoglobin none Bilirubin none to trace pH 4.6 – 8.2 (avg. 6.0) Ketones none 2 7. Chloride – normal value 10-12g/24hr. Chloride urinary content reflects the intake of dietary NaCl. 8. Total Solids (TS) – The daily urine output contain: water organic solute NPN compounds urea – 90% uric acid creatinine urobilinogen inorganic solute Na+ C1Ca++ PO4= K+ SO2= NH4+ Normal value 40-60g/24 hr Microscopic Tests 9. Microscopic Analysis – of the urinary sediment helps detects kidney disease. Normal urine contains epithelial cells, organic and inorganic crystals which reflect diet, mucus, a small number of red and white cells. Casts may also be seen. Casts are cylindrical structures molded to the wall of the renal tubule from a gel of protein in the urine. Hyaline (translucent) casts appear sometime in urine of healthy persons. The continual presence of casts indicates renal disease. The presence of casts in the urinary sediment is also accompanied by protein in the urine. 3