Hookworms
advertisement

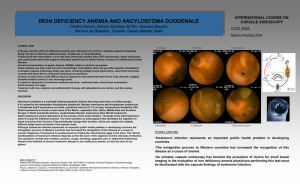
Hookworms The hookworms live in the upper part of small intestine. They feed on the blood and cause hookworm disease, which is one of the five major parasitic diseases in China. Two species, Ancylostoma duodenale(十二指肠 钩口线虫)and Necator americanus(美洲板口线虫), are prevalent in our country. I. Morphology 1. Adults: They look like an odd piece of thread and average about 1cm. They are white or light pinkish when living. Their strong mouth cavities are armed with teeth or cutting plates. The female is slightly larger than the male. The male’s posterior end is expanded to form a copulatory bursa. Morphological Differences between Two Species of Hookworms —————————————————――—————————— A. duodenale N. americanus ———————————————————――————————— Size about 1 cm, larger smaller ————————————————————――———————— Shape single curve, looks like“C” double curves, looks like“S” —————————————————————――——————— Mouth 2 pairs of ventral teeth 1 pair of ventral cutting plates ——————————————————————――—————— ♂Copulatory 1 pair with separate 1 pair which unite to form Spicule endings a terminal hooklet ———————————————————————――————— ♀caudal spine present no ————————————————————————――———— ♀vulva position post-equatorial pre-equatorial —————————————————————————――——— 2. Egg: 60×40μm, oval, shell is thin and colorless, content is 2-8 cells. Differences between Decorticated Ascaris and Hookworm eggs -———————————————————————————— Decorticated ascaris egg hookworm egg —-——————————————————————————— Shell thick thin ——-—————————————————————————— Egg cell unsegmented 4-8cells ———――———————————————————————— Space between shell and cell new-moon shaped space between cell and ends of shell empty space surrounding the segmented cells ———――———————————————————————— II. Life Cycle 1.Geohelminth, 2.Final host: man, 3.Inf. Stage: Larva 3 or filariform larva, 4.Inf. Route: by skin, 5. Feeding habits: blood, 6. Blood loss: 0.02~0.1ml/Na/day;(0.02~0.1) × 7 ml/Ad/day, 7. Site of inhabitation: upper part of small intestine, 8. Life span: average 3 years, Ad 7 years, Na 15 years, 9. Egg output: 10,000~30,000/Ad/day;5000~10,000/Na/day, 10. Blood-lung migration: skin—venacava—right heart—lungs **Question: How many differences are there between the life cycles of Ascaris and Hookworm? Filariform heart------- penetrate skin larvae-------------------------------Venacava--------via vessels or Right lymphatics expectoration---death Lungs (alveolus, bronchiole, bronchus)-----Trachea-----Pharynx---------------molt 3,4 Passed in feces swallowed Duodenum----------- ♀ ♂ Adults-------Eggs ------------------ Outer environment 20-30℃, humidity 80% -----------------------------out---------------24hrs Rhabditiform molt2 Rhabditiform larvae molt 1, 48hrs 1(L1) hatching survive 15wks in moist soil larvae2(L2)---------Filariaeform larvae (L3)------------------------Waiting for the host in soil or on grass or crop whole process 5-7weeks III. Pathogenesis and Clinical Manifestations 1. Larval migration phase (1) Dermatitis is also known as "ground itch" or "stool poison". The larval penetration of skin causes a locally allergic reaction, the petechiae(瘀 点)with an itching and burning sensation. Scratching leads to secondary infection. The skin lesions heal within 2 weeks. (2) Pneumonitis (allergic reaction; Loeffler's syndrome): The migrating larvae damage the alveolar capillaries and patients manifest cough, asthma, low fever, blood-tinged sputum or hemoptysis ( 咯 血 ) , chest-pain, inflammation shadows in lungs under X-ray and eosinophilia(嗜酸性粒细 胞增多). These manifestations go on about 2 weeks. 2. Adults in small intestine (1) A large worm burden results in microcytic hypochromatic anemia (*characteristic manifestation). The symptoms are lassitude, edema, palpitation of the heart. In severe case, death may result from cardiac failure or physical exhaustion. **The anemia results from hookworms sucking blood and excessive blood loss. The excessive blood loss is due to the large worm burden; worms secreting several antiagglutinating materials (antiagglutinin 抗凝素, and etc.), often changing the place to suck blood and discharging undigested blood; the old injured sites of the intestinal wall continuing to bleed. The other reason for the anemia is that the patient can not get enough noutrition. (2) Allotriophagy ( allotriophagia, geophagia or pica 异嗜症) is due to the lack of trace element iron (ferrum) (3) Epigastric pain as that of a duodenal ulcer; dearrhea. (4) Amenorrhea, sterility, abortion may occur in the women. (5) Gastrointestinal bleeding (6) Infantile hookworm disease IV. Diagnosis Diagnostic criterion: 1. hemoglobin is lower than 12g/dl in man, 11g/dl in woman. 2. find hookworm eggs. Method: 1. saturated brine flotation technique is first choice. 2. direct fecal smear 3. larval culture V. Treatment & Prevention 1. Albendazole or Mebendazole; 2. Avoid the skin contacting with the infective larvae in soil or on plants. VI. Epidemiology Both species of hookworm are prevalent in the tropics and subtropics. The optimal temperature for Ancylostoma duodenale is 22-26 ℃ , so Ancylostoma duodenale is mainly prevalent in the north of China. Necator americanus is mainly distributed in the south of China due to it prefer the temperature of 31-35℃. *Factors favoring the hookworms spread: 1. Simple life cycle (geohelminth). 2. Pollution of the soil by human feces containing enormous hookworm eggs. 3. Warm and moisture climate is favorable for the development of hookworm eggs and larvae. 4. Human gets infection by the skin contacting with the infective larvae in fertilized soil or on plants. The hookworm incidence of barefoot farmers is the highest. VII. Prevention Unified measures: 1. Sanitary disposal of night soil, 2. Individual protection, 3. Health education, 4. Cultivating hygienic habits, 5. Treatment of the patients and carriers. Enterobius vermicularis (pinworm) It is commonly found infecting humans, especially in children. The adult worms inhabit the cecum and adjacent intestinal lumen. Right after mating, the male dies. Therefore, the male worms are rarely seen. The female worms migrate down the intestinal tract. At midnight, when the anal sphincter is relaxed, the worms migrate out the anus depositing eggs on the perianal skin and causing perianal itch. Humans get the infection by mouth or retro-infection, and by the mode of auto-infection or foreign infection. It is commonly found in kindergarten and primary school students. I. Morphology The female adult looks like a pin, measures about 1 cm and is white in color. The fusiform body terminates in a long, thin, tapering tail. The anterior end tapers and is flanked on each side by cuticular extensions called “alae”(颈翼). The esophagus terminates in a prominent muscular bulb (esophagus bulb 食道球). The male adult is only about one-third to one-half the size of a female and has a curled tail. The eggs are persimmon seed-like, about 55×25 m. it is clear, colorless and contains a larva. II. Life cycle 1. Site of inhabitation: ileocecum; 2. Infective stage: embryonated eggs; 3. Source of infection: auto-infection and foreign infection; 5.Inf. route: by mouth or by retro-infection; 5. No intermediate and reservoir hosts; 6. Egg output: 5,000-15,000/♀/a life; 7. Life span: ♀1 month; 8. Feeding habits: blood, tissue fluid and intestinal contents; 9. Site of oviposition: perianal skin. Migrates out anus 35℃, humidity 95%, 6hrs Pregnant♀----------------------eggs ---------------------------Embryonate eggs At mid night, deposits perianal skin swallowed by man -----------------------Larvae intestine-----------------cecum-----or retro-infection ♀♂adults mate migrate down hatching out in (2-6 wks) III. Symptomatology About one-third of pinworm-infected persons are asymptomatic. The major symptom, anal itch, is associated with the nocturnal migration of the gravid females from the anus and deposition of eggs in the perianal folds of the skin. (1) In children: Anal pruritus (anal itch) results in scratching anus, restlessness, grinding their teeth in sleep, nervousness, irritability, divided attention and poor school record. (2) Ectopic injure: In young girls, migration of the worms may produce vaginitis, urethritis, and rarely peritonitis, egg granuloma of abdominal cavity, salpingitis giving rise to sterility. IV. Diagnosis *Cellophane tape technique is first choice. *The examination should be made in the morning, before the patient has not washed the anus or defecated. V. Treatment and Prevention 1. Albendazole or Mebendazole is very effective. Since the life span of the pinworm is about one month, the major problem is re-infection. Repeated treatment may be necessary for a radical cure. 2. Carry out the general survey and treatment. 3. Carry out the health education and cultivate hygienic habits VI. Epidemiology Enterobiasis is widely prevalent all over the world even in cold or developed countries. Its epidemiological characteristics include that the incidence is higher in children than adults; it is most common where people live under crowded conditions such as orphanages, kindergartens, refugee camps and large families; the infection and re-infection are very easy due to the simple life cycle and the infective route of anus-fingers-mouth.. Question: What are enterobiasis? the epidemiological characteristics of