Montefiore Medical Center
advertisement

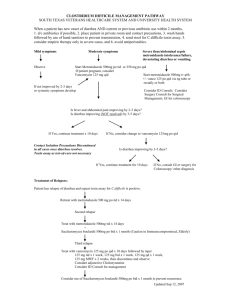
Montefiore Medical Center Moses/Einstein Divisions C. Difficile Colitis Treatment Guidelines 1. Stop antibiotics whenever possible. 2. Avoid antiperistaltic agents such as loperamide. Decrease the usage of antimotility medications such as morphine and its analogues. 3. Initial treatment: Patients with mild-to-moderate illness: - metronidazole 500mg PO/IV q8h x 10-14 days is recommended. (Vancomycin 125mg PO q6h may be used as 1st line therapy for C. difficile associated diarrhea/colitis if the patient: 1) develops C. difficile colitis while on metronidazole; 2) is allergic or intolerant to metronidazole; 3) is pregnant Patients critically ill* or not responding to metronidazole within 72 hours of treatment: - vancomycin 125-250mg PO q6h is recommended. - surgical evaluation should be considered. (*Critically ill is defined as: severe abdominal pain/tenderness/distention, temp >101°F, albumin <2.5 mg/dl, WBC >20K, decreasing bicarbonate, rising creatinine, age >60) 4. Treatment of recurrence: 1st recurrence: - repeat 2nd course of treatment with the same drug (either metronidazole or vancomycin as used for initial treatment). Multiple recurrences (ID or GI should be consulted): - tapered or pulsed doses of PO vancomycin should be considered. Week 1: 125-250mg PO q6h Week 2: 125-250mg PO q8h Week 3: 125-250mg PO q12h Week 4: 125-250mg PO daily Week 5, 6: 125-250mg PO every other day Week 7, 8: 125-250mg PO every 3 days - after the 2nd recurrence, adjunctive therapy with probiotics such as Saccharomyces boulardii may be considered. Please note: Dual therapy with PO vancomycin and PO metronidazole has no proven additional benefit. Dual therapy may be used if the patient has an ileus or gastroparesis; vancomycin enema + IV metronidazole may be an option (PO vancomycin is not appropriate). Dual therapy with PO vancomycin and IV metronidazole may be used in patients who have severe or complicated C. difficile associated diarrhea/colitis. IV vancomycin is not efficacious for the treatment of C. difficile associated diarrhea/colitis. Cholestyramine binds to a variety of drugs in the GI tract including vancomycin, thereby rendering effective agents potentially ineffective. Efficacy data for cholestyramine is questionable. Presently, there are not enough clinical data to support the routine use of nitazoxanide (non-formulary), rifampin and rifaximin in the treatment of C. difficile associated diarrhea/colitis. When clinical picture indicates C.difficile disease, but toxin tests are negative, contact Microbiology Laboratory (ext. 4695) for additional tests. Guideline prepared by representatives from Gastroenterology, Infectious Diseases, Microbiology, Pharmacy and Surgery.