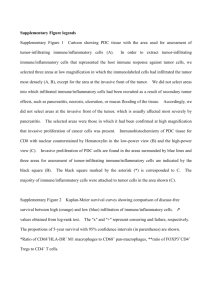
2011 - The Waddensymposium
advertisement

Final program of the 4th Waddensymposium organized by the Department of Immunohematology and Blood Transfusion of the LUMC. Location: Grand Hotel Opduin Ruijslaan 22 1796 AD De Koog (Texel) The Netherlands Department of Immunohematology and Blood Transfusion Symposium secretariat: Amber Günthardt Mail: a.n.gunthardt@lumc.nl Phone: +31 71 526 38 27 Organizing committee: Ferry Ossendorp Sjoerd vd Burg Wim Fibbe John Haanen Kees Melief Jaap Oostendorp Jaap Jan Zwaginga th 4 Waddensymposium on Novel strategies in immunotherapy of cancer This symposium is organized in collaboration with: ` www.waddensymposium.eu Location: Grand Hotel Opduin, Texel, the Netherlands www.opduin.nl Final program, 26th of June till the 29th of June 2011 Sunday 26th of June 18.00 Arrival Hotel Opduin, Texel 20.00 Dinner Monday 27th of June 07.30 - 08.15 Breakfast 08.15 - 08.30 Welcome, symposium in perspective: Willem Fibbe, Leiden [The Netherlands] Molecular targeting Chair: Ferry Ossendorp 08.30 – 09.05 Michel C. Nussenzweig [USA] ”DC routing” 09.05 – 09.40 Yvette van Kooyk [The Netherlands] “Glycan modification of antigens for potentiating anti-tumor immunity” 09.40 – 10.15 Günther Hartmann [Germany] “RIG-I mediated immune activation” 10.15 – 10.50 Jacques Neefjes [The Netherlands] “How Doxorubicin alters the transciptome and MHC class I peptidome: Consequences for tumor immunotherapy” 10.50 – 11.20 Coffee break 11.20 – 11.55 Maries van den Broek [Switzerland] “Local radiotherapy promotes tumour-specific CD8-effector function through DC activation” 11.55 – 12.55 Short abstracts Wendy Unger, Jasper van den Boorn, Petra Paul, Thorbald van Hall, Claudia Cunha Oliveira, Gijs Zom, Rodney Rosalia, Joost van den Berg 13.00 – 13.45 Lunch 14.00 – 18.00 Informal discussion between young talented scientists / invited speakers (Transfer at 14.00h) 18.00 – 20.00 Dinner 20.00 – 21.00 Keynote lecture Chair: Jaap Oostendorp Axel Hoos [USA] “Accelerating innovation of cancer immunotherapies” Tuesday 28th of June 07.30 – 08.30 Breakfast Preclinical models Chair: Sjoerd van der Burg 08.30 – 09.05 Thomas Kündig [Switzerland] “Intralymphatic Immunotherapy” 09.05 – 09.40 Per Thor Straten [Denmark] “CD8 T cells in cancer; killers, supporters and suppressors” 09.40 – 10.15 Vincenzo Bronte [Italy] “Chemokine nitration prevents intratumoral infiltration of antigen- specific T cells” 10.15 – 10.45 Coffee break 10.45 – 11.20 Pam Sharma [USA] “Targeting the ICOS/ICOSL pathway for improved anti-tumor responses” 11.20 – 11.55 Linda Sherman [USA] “New roles for CD4 help in the tumor environment” 11.55 - 12.30 Frances Balkwill [UK] “Inflammatory cytokines and autocrine tumour-promoting networks in human ovarian cancer” 12.30 – 13.00 Short abstracts Rinke Bos, Moniek Heusinkveld, Marleen van Loenen, Daniel Hirshhorn 13.00 – 13.30 Lunch 13.45 – 18.00 Informal discussion between young talented scientists / invited speakers (Transfer at 13.45h) 18.00 – 20.00 Dinner 20.00 – 21.00 Keynote lecture Chair: Kees Melief Jim Allison [USA] “Anti-CTLA-4 treatment in cancer” Wednesday 29th of June 07.30 – 08.30 Breakfast Clinical application Chair: John Haanen 08.30 – 09.05 Glenn Dranoff [USA] “Mechanisms of Protective Tumor Immunity” 09.05 – 09.40 Jolanda de Vries [The Netherlands] “The potency of human plasmacytoid dendritic cells to induce immune responses in melanoma patients” 09.40 – 10.15 Christian Ottensmeier [UK] “DNA vaccination against cancer” 10.15 – 11.15 Short abstracts Marij Welters-Schoenmaekers, Gerty Schreibelt, Stefan Nierkens, Pauline Meij, Tetje van der Sluis, Marieke Fransen, Pia Kvistborg, Marcelo Navarrete 11.15 – 11.45 Coffee break 11.45 – 12.45 General discussion and position paper 12.45 – 13.30 Lunch 13.35 Departure by bus to Harbour 14.00 Departure boat to Den Helder END OF MEETING ABSTRACTS MONDAY Glycan modification of antigens for potentiating anti-tumor immunity Ingeborg Streng-Ouwehand, Manja Litjesn, Astrid van Beelen, Hakan Kalay, Sven Bruijns, Wendy Unger, and Yvette van Kooyk Dendritic cells (DC) are specialized in the recognition of pathogens and play a pivotal role in the control of immunity. Yet DCs are also important for homeostatic control recognizing self antigens and tolerizing its environment, indicating that the nature of the antigen it recognizes may steer a DC towards immunity or tolerance. DC express several C-type lectins, that function as innate receptors that recognize pathogens, and facilitate antigen uptake and presentation. Yet many of these receptors also modify responses through signalling interference with TLR. We and others have shown that the C-type lectins DC-SIGN, MGL and Siglecs recognize specific glycan structures on many pathogens, and modulate DC mediated responses. Our data demonstrate that the glycan composition of the pathogens plays a dominating role in directing the immune response of DC. Recently we started to modify antigens with specific glycans to favour direction of antigens to DC, in particular to these specific antigen uptake receptors to allow processing of antigen for presentation to T cells. Glycan modification of antigen with DC-SIGN or MGL binding glycans can strongly affect the antigen uptake and presentation capacity of DC and instruct antigen specific CD4 and CD8 T cell responses and Th1 differentiation. We have shown that uptake of specific glycosylated antigen is differently routed intracellularly and favors cross presentation without the need of any TLR signalling. We show that glycan modified antigens as protein/peptide or particulate compositions targets these innate receptors on DC which leads to tailored immune responses both in-vitro and in-vivo that may control immunity against cancer and infectious diseases. MONDAY RIG-I-mediated immune activation Günther Hartmann The innate immune system detects viruses based on the recognition of viral nucleic acids. Immunorecognition of viral nucleic acids leads to the initiation of early antiviral immune responses that limit viral replication and are essential for eliciting acquired immune responses to virus specific antigens. Detection of viral nucleic acids in the cytosol is based on the family of the so-called RIG-I-like receptors (RLRs). RNA with a triphosphate group at the 5´end (3pRNA) is the ligand for RIG-I (1). By using a new chemical approach for 5´triphosphate oligoribonucleotide synthesis we found that short double strand conformation with base pairing of the nucleoside carrying the 5´triphosphate is required for RIG-I binding. These results explain how RIG-I detects negative strand RNA viruses which lack long double-stranded RNA but do contain panhandle blunt short double-stranded 5´triphosphate RNA in their single-stranded genome (2). The crystal structure of the RIG-I CTD domain bound to the blunt-end of a 5’-ppp-dsRNA was resolved. The structure, supported by mutation and functional studies, defines how a lysine-rich basic cleft within the RIG-I CTD domain sequesters the 5’-ppp end of the bound RNA (3). We found that a conserved histidine in RIG-I controls immune tolerance of 2′O-methylated cap1 self RNA. Furthermore we demonstrate that RIG-I-RNA ligand interaction not only activates type I IFN, but also induces inflammasome activation (4) and pro-apoptotic signaling (5). Based on these activities, RIG-I ligands are promising candidates for the therapy of viral infection and cancer. We developed short interfering RNA (siRNA) containing triphosphate groups at the 5´ends (3p-siRNA) targeting oncogenes (6) and designed potent RIG-I selective ligands for tumor therapy. 1. Hornung V, … and Hartmann G. 5'-Triphosphate RNA Is the Ligand for RIG-I. Science 2006; Nov 10; 314:994-7. 2. Schlee M, … and Hartmann G. Recognition of 5´-triphosphate by RIG-I helicase requires short blunt double-stranded RNA as contained in panhandle of negative strand virus. Immunity 2009, 31:25-34. 3. Wang Y, Ludwig J, ...Tuschl T°, Hartmann G°, Patel DJ°. 2010. Structural and functional insights into 5'-ppp RNA pattern recognition by the innate immune receptor RIG-I. Nat Struct Mol Biol 2010;17:781-7. °equally contributed 4. Poeck H, ... Hartmann G°, Hornung V°, Ruland J°. Recognition of RNA virus by RIG-I results in activation of CARD9 and inflammasome signaling for interleukin 1 beta production. Nat Immunol. 2010;11:63-9. °equally contributed 5. Besch R, …and Hartmann G. Proapoptotic signalling by RIG-I and MDA-5 results in type I interferon independent apoptosis in melanoma. J Clin Invest 2009, 119:2399-411. 6. Poeck H, …and G Hartmann. 5´-triphosphate-siRNA: turning gene silencing and RIG-I activation against melanoma. Nature Medicine 2008; 14:1256-63. MONDAY How Doxorubicin alters the transciptome and MHC Class I peptidome: Consequences for tumor immunotherapy Jacques Neefjes Tumor Immunotherapy responses can be boosted by combining treatment with radiotherapy and/or chemotherapy. Radiotherapy activates locally the mTOR pathway that enhances translation and generates more peptides for MHC class I molecules (Reits et al., 2006). A frequently used drug in oncology is the topo-isomerase II inhibitor doxorubicin that is more effective that etoposide, another topo-II inhibitor. We will show how doxorubicin selectively alters the epigenetic code in areas of open chromatin that are abundantly present in immune and in tumor cells. This has marked effects on transcription over long periods and alters the peptidome in MHC class I molecules such that selective elimination can be improved. Understanding the biology of these cancer compounds will rationalize the application in immunotherapy of cancer MONDAY Radiotherapy promotes tumour-specific effector CD8+ T cells via DC activation Anurag Gupta, Hans Christian Probst, Van Vuong, Alexandro Landshammer, Sabine Muth, Silvia Behnke, Reto Schwendener, Martin Pruschy, Alexander Knuth, Maries van den Broek Radiotherapy is an important treatment for cancer. The main mode of action is thought to be the irreversible damage to tumour cell DNA, but there is evidence that irradiation mobilizes tumour-specific immunity and recent studies showed that the efficacy of ablative radiotherapy depends on the presence of CD8+ T cells. We show here that the efficacy of ablative radiotherapy crucially depends on dendritic cells and CD8+ T cells, whereas CD4+ T cells or macrophages are dispensable. We show that local ablative irradiation results in activation of tumour-associated dendritic cells that in turn support the development and local survival of tumor-specific effector CD8+ T cells as well as the maintenance of their local effector function. We propose that – in the absence of irradiation – the activation status of dendritic cells rather than the amount of tumour-derived antigen or frequency of tumour-specific CD8+ T cells is the bottleneck, which precludes efficient anti-tumour immunity. MONDAY Sialic acids on (tumor)antigens induce tolerance via modulation of dendritic cells Wendy Unger, Maurizio Perdicchio, Marleen Verstege, Martino Ambrosini and Yvette van Kooyk Sialic acids (SA) are the most prevalent terminal monosaccharides on cell surface glycoproteins and connected to the underlying glycan-core structure by different linkages like 2,3 (SA-2,3) and 2,6 (SA-2,6). Increased expression of SA is related to invasion and metastasis of tumors such as melanoma and colon cancer. These tumors are also associated with high frequencies of tumorantigen-specific regulatory T-cells (Treg). Since hypersialylation of certain bacteria is often linked to immune evasion, we hypothesized that SA on tumor cells dampen anti-tumor immune responses by modulation of antigen-sampling dendritic cells (DC). We set out to link either SA-2,3 or SA-2,6 to the model antigen OVA to assess their effect on murine BMDC as well as OVA-specific T-cell responses. Compared to native OVA, the uptake of the glycoconjugates was increased; however, this did not result in increased MHC class-II antigen presentation as proliferation of OT-II T-cells was similar. Native OVA targeted BMDC induced Th1 development, especially when adjuvants were co-administered. By contrast, OVA-SA-2,3 and OVA-SA-2,6 targeted BMDC drive the differentiation of naïve T-cells into FoxP3+ Treg, which suppress the proliferation of responder T-cells. We are currently investigating the phenotype of the BMDC incubated with the different glyco-antigens and whether SA on murine melanoma cells drive Treg generation via modulation of DC in-vivo. MONDAY Monobenzone-induced immune attack of pigmented cells Jasper G. van den Boorn, Cornelis J. Melief, Rosalie M. Luiten Monobenzone is a phenolic compound with the capacity to induce progressive skin depigmentation that is clinically and histologically indistinguishable from vitiligo vulgaris. The exact mode of action by which monobenzone induces vitiligo has remained unknown. Recently we have shown that monobenzone specifically endows exposed pigmented cells with immunogenicity. Using autologous healthy human donor DC-T cell stimulations, we established that monobenzone-exposed melanoma cells induced a robust melanoma-reactive CD8+ T cell response in vitro within 7 days, as compared to unexposed melanoma cells. Importantly, 78% of the melanoma cell-reactive CD8+ T cell clones generated with monobenzone were found to recognize monobenzone-treated and –untreated melanoma cells equally well. Furthermore we have found that upon enzymatic conversion of monobenzone by the melanosomal enzyme tyrosinase, the quinone metabolites resulting from this reaction form haptens specifically to cysteine residues in proteins. Moreover, this enzymatic conversion was found to generate reactive oxygen species, induce melanosome autophagy and mediate the release of tyrosinase- and MART-1-containing CD63+ exosomes from monobenzone-exposed pigmented cells. Moreover, monobenzoneexposed pigmented cells activated dendritic cells. These data show that monobenzone, by its specific effects on the enzyme tyrosinase, induces potent CD8+ T cell immunity against auto-antigens expressed by melanocytes and melanoma cells. Monobenzone thereby presents a powerful new drug in the field of melanoma immunotherapy. This research was funded by an innovational research grant of the Netherlands Organisation of Scientific Research (NWO-vidi). MONDAY A Genome-wide Multi-Dimensional RNAi Screen Reveals Pathways Controlling MHC Class II Antigen Presentation Petra Paul, Tineke van den Hoorn, Marlieke Jongsma and Jacques Neefjes MHC class II molecules present antigenic peptides to T helper cells to facilitate immunity against pathogens and are strongly linked to autoimmune diseases. To unravel processes controlling MHC class II antigen presentation, we performed a genome-wide flow cytometry-based RNAi screen detecting MHC class II expression and peptide loading. The 276 hits were subjected to two additional high-throughput assays. We identified nine regulators of MHC class II gene transcription acting in complex feedback networks controlled by chromatin modification, pathogens, TGF and other signalling events. Phenotypic clustering of the intracellular distribution of MHC class II located a new GTPase, FLJ22595/ARL14, on MIICs. Integration of functional and gene expression datasets identified five novel proteins, including FLJ22595/ARL14, which control MHC class II transport in dendritic cells. The results represent the first genome-wide functional analysis of a critical immunological process – MHC class II antigen presentation – and identify new pathways and targets for manipulating immune responses. MONDAY A novel category of tumor antigens enable CTL immunity to tumor escape variants. Thorbald van Hall Loss of antigen presentation by MHC I constitutes a major escape mechanisms by tumors and allows them to escape elimination by cytotoxic T-lymphocytes. Recently, we identified a novel category of tumor antigens that are selectively presented by such tumor variants and named them TEIPP (T cell epitopes associated with peptide processing)*. TEIPP antigens are derived from housekeeping proteins, but are surprisingly not presented in MHC I under normal conditions. Multiple defects in the antigen presentation pathway, e.g. TAP or tapasin, drive the emergence of these peptides at the cell surface. A broad and cytotoxic CD8+ T cell population recognizes these as neo-epitopes in the context of classical MHC I molecules. Interestingly, we found that a major fraction of TEIPP T cells are restricted by the non-classical MHC Qa-1b, which is the mouse homolog of HLA-E. This non-polymorphic molecule normally accommodates monomorphic signal peptides and functions as a ligand for germ-line receptors CD94/NKG2 on NK cells. We now found that this conserved peptide is replaced by a novel peptide repertoire of surprising diversity as a result of impairments in the antigen processing pathway. The surprising absence of TEIPP peptides from normal cells was not related to weak binding or stability of the Trh4/Db complexes, or to limited availability of MHC-I heavy chains, but rather to expression levels of the antigen. Strongly augmented expression levels of Trh4 were needed to reach comparable peptide display as on TAP-deficient cells, suggesting that the influx of TAP-transported peptides in the ER forms an efficient barrier for peptides from alternative processing routes. Finally, we demonstrated that TEIPP T cell responses can easily be detected in humans and revealed the identity of the first human TEIPP. Thus, therapeutic application of classical and non-classical TEIPP antigens might enable the CTL-mediated elimination of tumors with MHC I presentation defects to prevent this type of immune escape. * Nat Med 12:417, 2006; J Immunol 178:657, 2007; Canc Res 67:8450, 2007; J Exp Med 207:207, 2010; J Immunol 185:6508, 2010. Cur Op Immunol 23:293, 2011. MONDAY Peptide transporter TAP mediates between competing sources of MHC-I peptides. Cláudia C. Oliveira, Bianca Querido, Marjolein Sluijter, Sjoerd H. van der Burg and Thorbald van Hall Defects in the intracellular peptide transporter TAP in tumors are associated with immune evasion. Recently, we described a category of TAP-independent peptides that fail to be presented by normal processing-intact cells, but are only displayed on cells with deficiency in the classical MHC-I pathway. Tumor cells presenting TAPindependent peptides can be targeted and eliminated by specific CD8+ T cells. We studied the ubiquitously expressed ceramide synthase Trh4 as a prototypic example of these neo-antigens and found that partial inhibition of TAP function allows for cell surface presentation of Trh4 peptide/Db complexes. These partially inhibited cells exhibited a mixture of TAP-dependent and TAP-independent peptide repertoires, indicating that TAP operates as a lever of control that determines relative contributions of both peptide repertoires. The absence of the Trh4 peptide from normal cells was not related to binding or stability of Trh4/Db complexes, or to limited availability of MHC-I heavy chains, but rather to expression levels of the antigen, since increased expression of Trh4 induced peptide presentation on processing-intact cells. However, high expression levels were needed to reach comparable peptide display as on TAP-deficient cells, indicating that the ER influx of TAP-transported peptides forms an efficient barrier for peptides from other processing routes. Decreased TAP function, as commonly found in cancers and virus-infected cells, alleviates this barrier and results in the co-presentation of this TAP-independent peptide repertoire. This repertoire might constitute an important line of host defense suitable to be exploited in therapeutic intervention strategies. MONDAY Efficient induction of anti-tumor immunity by Toll-like receptor ligand-peptide conjugates Zom GGP, Khan S, Britten CM, Sommandas V, Camps MGM, Loof NM, Meeuwenoord NJ, Filippov DV, Van der Marel GA, Overkleeft HS, Melief CJM, Ossendorp F Chemical conjugates comprising synthetic Toll-like receptor ligands (TLR-L) covalently bound to synthetic antigenic peptides are an attractive vaccine modality that can induce a robust CD8+ T-cell immune response. We have previously shown that the mechanism underlying the improved power of conjugates compared to mixtures of peptides and TLR ligands, depends on improved delivery of the antigen together with a dendritic cell (DC) activation signal. In the present study we show that Toll-like receptor peptide conjugates (TPC) have superior capacity of T-cell priming compared to free synthetic peptide injected together with a free TLR-ligand. Importantly, we observed that prophylactic immunization with TPC leads to efficient induction of tumor protection in mice challenged with aggressive tumors such as B16 F10 Ovalbumine transduced melanoma and RMA lymphoma. In addition, our data show that both CD4 and CD8 T-cell responses are required for the anti-tumoral effects. Collectively, these data show that TPC are promising, fully synthetic, vaccine candidates. MONDAY Encapsulation of protein antigen in nanoparticles induces potent CD8+ T cells in vitro with improved anti-tumor effector function and persistence in peripheral blood after adoptive transfer. Rodney A Rosalia, Ana Luisa Silva, Ahmed Allam, Selina Khan, Sjoerd van der Burg, Wim Jiskoot, Ferry Ossendorp, Jaap Oostendorp Potent effector CD8+ T cells are vital in anti-tumor immune responses as they are capable of direct recognition and cytotoxicity of malignant cells. Protein antigens aimed at activating CD8+ T cells have so far yielded disappointing results due to poor efficiency of cross-presentation of soluble protein by Dendritic cells (DC). Deficient cross-presentation of protein antigens results in sub-optimal priming and activation of CD8+ effector T cells. Therefore, alternative strategies need to be developed to improve specific cellular immune responses induced by protein antigens. In the present study we have applied Poly-Lactic-co-Glycolic-Acid (PLGA)nanoparticles containing Ovalbumin (OVA) (PLGA-OVA) as an antigen-delivery system to improve crosspresentation of soluble proteins by DC. Optimal Ag crosspresentation was achieved with 100-fold lower PLGA-OVA amounts compared to soluble OVA (sOVA). Improved Ag crosspresentation by DC resulted in efficient priming of CD8+ T cells inducing highly activated CD69-positive, IFN-γ and IL-2 producing CD8+ T cells. Adoptive transfer of in vitro primed CD8+ T cells showed better antigen-specific in vivo cytotoxicity, longer persistence in peripheral blood, higher memory T cell formation and ultimately better capacity to protect animals from s.c. tumor challenge in comparison to T cells stimulated with DC loaded with sOVA. Therefore, we conclude that PLGA-encapsulation of protein antigen is a very efficient way to transfer protein antigen in cross-presentation pathways. Enhanced Ag crosspresentation led to potent CD8+activation with strong anti-tumor effector function upon adoptive transfer. MONDAY Genetic manipulation of tumor infiltrating lymphocytes from melanoma Joost H. van den Berg & Per Thor Straten Adoptive cell transfer (ACT) is a promising immunotherapeutic treatment possibility for disseminated cancer. ACT of high numbers of tumor infiltrating lymphocytes (TIL) results in objective response rates above 50% in heavily pretreated melanoma patients. Nevertheless, only a small fraction of adoptively transferred T lymphocytes is able to reach the tumor site once re-infused into the body. This project aims to improve the homing capacity of T lymphocytes towards the tumor site, which can possibly make ACT more efficient in a larger fraction of patients. Melanoma tumors secrete several chemokines which play an important role in tumor growth and metastasis. These chemokines can be utilized to increase the homing capacity of T lymphocytes towards the tumor micro-environment. In this project, in vitro expanded TIL cultures will be equipped with the chemokine receptor CXCR2 using mRNA electroporation. CXCR2 is the receptor for IL-8 and gro-α, two chemokines that are produced by the majority of melanomas. Electroporation will lead to transient chemokine receptor expression, sufficient to improve homing towards chemokine secreting tumors, without the risk of insertional mutagenesis associated with viral transductions. We have successfully established a mRNA electroporation protocol to express CXCR2 on patient derived TIL cultures. Electroporation results in high transfection efficiencies of the receptor (>90%) with no increase in cell death and preservation of killing capacity against a tumor antigen. Using a trans-well assay, we showed that CXCR2 transfected T lymphocytes have an improved in vitro migration capacity towards recombinant IL-8 and gro-α. In the next phase of this project, the in vivo homing capacity of transfected T cells towards melanoma will be evaluated in murine models. TUESDAY Intralymphatic Immunotherapy Thomas M. Kündig The immune response is initiated by dendritic cells (DCs) and other antigenpresenting cells. These cells are present in nearly all organs and tissues of the body, so that from an immunological perspective any organ or tissue could serve as a route for vaccine administration. The choice of route is therefore typically based on practical aspects. Using conventional needle and syringe the subcutaneous or intramuscular route are standard. The dermis and especially the epidermis are technically more difficult to target, but are likely to gain more interest due to the recent development of micro-needle patches and needle free injection devices. Vaccine administration via mucosal surfaces such as nasal or oral vaccination represents another option for needle free vaccine administration. While all these routes of administration have been proven to work and protect against childhood diseases, influenza and many other infectious agents, the discussion and comparison of these different routes usually focuses on convenience, reduction of pain and distress for children, cost and on the possibility for mass vaccination. Our research focuses on how the route of administration can enhance the efficacy of vaccination. Especially in therapeutic vaccination, i.e., in a smaller patient number that already suffers from a disease, vaccination efficiency rather than convenience is the main issue. This is particularly the case in therapeutic cancer vaccines and in allergen specific immunotherapy. Intralymphatic vaccination maximizes the efficacy of vaccines based on peptides, proteins, DNA and RNA, and the efficacy of adjuvants by several orders of magnitude. The presentation will focus on the history of this long known vaccination route, the types of vaccines that profit the most from intralymphatic administration, clinical applicability and results. TUESDAY CD8 T cells in cancer; killers, supporters, and suppressors Per Thor Straten We have characterized peptide antigens derived from proteins associated with crucial cancer traits, e.g., metastasis (RhoC), apoptosis (survivin, Bcl-2, Bcl-Xl, Mcl-1), and drug resistance (TRAG-3 and CYP1B1). Several of these antigens are in clinical testing (www.clinicaltrial.gov), however, vaccinations against cancer has so far not lived up to its promise, in part due to regulatory - or counter-active - mechanisms of the immune system. Heme-Oxygenase 1 (HO-1) and indoleamine 2,3-dioxygenase (IDO) are immune suppressive molecules expressed by cancer cells or by cells in the tumor microenvironment. We have characterized CD8 suppressor T cells specific for an HO-1 derived peptide and show that these T cells inhibit cytokine production, proliferation and cytoxicity. Importantly, some cancer patients harbour high frequencies of HO-1 specific T cells in their blood. Studying CD8 T cell responses to IDO derived peptides we demonstrate that IDO specific T cells can recognize and kill tumor cells as well as IDO-expressing dendritic cells and thereby unleash suppressed responses. A clinical trial is ongoing at our institution targeting IDO in patients with non small cell lung cancer. Another approach for harnessing the immune system to combat cancer is adoptive cell transfer (ACT) of in vitro expanded tumor infiltrating lymphocytes (TIL) – this treatment show promising clinical results in melanoma. However, the targets recognized by TIL is largely unknown. Using a combination of recently developed technologies for high-throughput analyses of T-cell responses and a compilation of all described melanoma antigens, we dissected the melanomarestricted T-cell responses found among TIL cultures. We show that different melanoma fragment-based cultures from the same patient present with very diverse characteristics in terms of T-cell specificities, and that tumor specific responses tend to decrease in frequency during rapid expansion. Surprisingly, the majority of detected responses are of very low frequency in percentage of CD8+ T cells. Thus, in terms of frequencies of tumor specific CD8 T cells the frequencies obtained by ACT seems not that different from vaccination induced responses. TUESDAY Targeting the ICOS/ICOSL pathway for improved anti-tumor responses Padmanee Sharma and James Allison Blockade of the T cell inhibitory molecule cytotoxic T lymphocyte antigen-4 (CTLA4) can lead to durable anti-tumor responses. A recent report documented an increase in survival of patients with advanced melanoma treated with Ipilimumab in a randomized placebo controlled Phase III trial, the first drug of any type to do so, with ~25% of patients alive for over 4 years after treatment. While this trial documents that CTLA-4 blockade can lead to clinical benefit, there is clearly a need to increase the numbers of patients who derive benefit from treatment. To investigate the immunologic impact of CTLA-4 blockade on human immune responses we conducted the first pre-surgical clinical trial with anti-CTLA-4 in patients with localized urothelial carcinoma of the bladder. Immunological analyses were conducted on tumor tissues and blood samples. We found an increased frequency of CD4 and CD8 T cells expressing high levels of the inducible costimulator (ICOS) molecule in tumor tissues of treated patients. The CD4+ICOShi population contained effector T cells that produced IFN- recognized the NY-ESO-1 antigen expressed on tumor cells. We therefore identified ICOS as marker of a subset of effector T cells that is increased after anti-CTLA-4 therapy. We also detected changes in tumor tissues consisting of increased T-bet and IFN- mRNA and an increased ratio of the Th1 cytokine IFN- to the Th2 cytokine IL-10, which was consistent with an increased ratio of ICOS-expressing effector to FOXP3-expressing regulatory T cells. Immunologic changes within tumors correlated with changes within peripheral blood in that an increased frequency of CD4+ICOShi T cells was also detectable in the systemic circulation of treated patients. We retrospectively examined peripheral blood samples from patients with metastatic melanoma who were treated with anti-CTLA-4 and found that sustained elevation of CD4+ICOShi T cells correlated with improved survival. These observations led us to test the possibility that engagement of ICOS could enhance the efficacy of anti-CTLA-4 therapy. To this end we transduced mouse B16F10 melanoma cells with a cDNA encoding ICOSL or a control construct. B16ICOSL+ cells (IVAX) and control B16 cells were irradiated and used alone or in combination with anti-CTLA-4 to treat mice bearing established B16F10 tumors. We found that combination of the IVAX with anti-CTLA-4 was markedly more effective than the control vaccine plus anti-CTLA-4 or that of any single treatment alone. The increase in therapeutic efficacy was accompanied by a marked in increase in the density and functionality of CD4 and CD8 T cells within the tumor. These results suggest a novel strategy for manipulating the immune system to enhance anti-tumor responses: checkpoint blockade coupled with provision of agonist signals to enhance costimulation mediated by ICOS. TUESDAY New Roles for CD4 help in the tumor environment Linda A Sherman CD4 help for CD8+ T lymphocytes prevents CD8 tolerance and promotes the survival of effector and memory CD8+ T cells. Although much is known about the benefits of CD4 help during CD8 priming, the role of CD4 help within the tumor microenvironment is less explored. Using a model in which tumor eradication by CD8+ T cells requires tumor specific CD4 help, we examined the basis for helper dependence of tumor eradication by CD8+ T cells. Recruitment of CD8+ T cells was greatly accelerated by production of IFN- resulted in the production of multiple chemokines in the tumor environment. Production of IL-2 by tumor resident CD4+ T cells enhanced CD8+ T cell proliferation and significantly upregulated the production of granzyme B required for tumor cell killing. These results highlight the importance of CD4 help in optimizing recruitment and effector function of CD8+ T cells within targeted tissues. TUESDAY Inflammatory cytokines and autocrine tumour-promoting networks in human ovarian cancer Frances Balkwill A complex network of inflammatory cytokines and chemokines regulates communication between the malignant cells and supporting stroma in most experimental and human cancers. There is ample evidence from animal models that individual members of this cytokine network and their intracellular signalling pathways can make malignant cells resistant to apoptosis, can stimulate a tumorpromoting leukocyte infiltrate that may also suppress anti- cancer immune responses, and can regulate angiogenesis. Of all the individual cytokines and chemokines that have been implicated in tumor growth and spread, the most convincing and extensive animal model data relate to the cytokines TNF-, IL-6 and the chemokine receptor CXCR4. These, and the CXCR4 ligand CXCL12, as well as the receptor Notch3 and its Jagged1 ligand, are coexpressed and co-regulated in ovarian cancer cell lines and human ovarian cancer biopsies. We have named this co-regulation the TNF network. High levels of expression of TNF network gene pathways in cell lines and ovarian cancer biopsies is significantly associated with pathways and process important to cancer growth and spread including angiogenesis, cell adhesion, stromal development, Notch signaling and the immune cell infiltrate. In ovarian cancer biopsies high levels of malignant cell staining for some TNF network members related to poor prognosis. To translate these observations to clinical practice, we have focused on IL-6. IL-6 is a major mediator of cancer-related inflammation in several cancers and promotes tumor growth and angiogenesis as well as evasion of apoptosis. We investigated the therapeutic activity of CNTO328 (siltuximab), an anti-human IL-6 antibody, in preclinical and clinical experiments. There was evidence of clinical activity of the anti-IL-6 antibody, with one patient of eighteen demonstrating a partial response and seven showing disease stabilisation for up to nine months. In terms of mechanism of action, the clinical, pre-clinical and in silico experiments showed that antibodies to IL-6 can have multiple actions within the tumor microenvironment in ovarian cancer including reductions in cytokine production, tumor angiogenesis and tumor macrophage infiltrate. We conclude that IL-6 is an important regulator of the tumour microenvironment in ovarian cancer and is a therapeutic target. TUESDAY CD4+ T cell help in the tumor milieu Rinke Bos and Linda Sherman CD4 help for CD8+ T lymphocytes prevents CD8 tolerance and promotes the survival of effector and memory CD8+ T cells. Using a murine model of spontaneous tumor formation in the pancreatic islets, RIP-Tag2HA, in which tumors express the hemagglutinin (HA) protein of influenza as a surrogate tumor antigen, we have described additional helper functions of tumor specific CD4+ T cells that require the presence of CD4 help within the tumor environment. Tumor resident CD4+ T cells accelerated the recruitment of CD8+ T cells through the IFN- of chemokines. Production of IL-2 by the tumor resident CD4+ T cells enhanced CD8+ T cell proliferation and also significantly upregulated the production of granzyme B. Elimination of either of these cytokines reduced tumor eradication and when both cytokines were absent, CD4 help was completely abrogated. We are now examining whether CD4 help can be replaced by systemic IL-2 treatment and what the effects are on CD8+ T cells in the tumor environment. All of these experiments have been performed with low-avidity CD8+ T cells and we are currently investigating whether high avidity CD8+ T cells will also benefit from CD4 help or whether the IL-2 production by the CD8+ T cells themselves is sufficient for efficient tumor killing. TUESDAY M2 macrophages induced by PgE2 and IL-6 from cervical carcinoma are switched to activated M1 macrophages by CD4+ Th1 cells Moniek Heusinkveld, Peggy J. de Vos van Steenwijk†, Renske Goedemans, Tamara H. Ramwadhdoebe, Arko Gorter‡, Marij J.P. Welters, Thorbald van Hall, Sjoerd H. van der Burg Monocytes attracted by tumor-induced chronic inflammation differentiate to antigenpresenting cells (APC), the type of which depends on cues in the local tumor milieu. Here, we studied the influence of human cervical cancer cells on monocyte differentiation and showed that the majority of cancer cells either hampered monocyte to DC differentiation or skewed their differentiation towards M2-like macrophages. Blocking studies revealed that M2-differentiation was caused by tumor-produced PgE2 and IL-6. TGF, IL-10, VEGF or M-CSF did not play a role. Notably, these CD14+CD163+ M2-macrophages were also detected in situ. Activation of cancer cellinduced M2-like macrophages by several TLR-agonists revealed that when compared to DC these M2-macrophages displayed a tolerogenic phenotype reflected by a lower expression of co-stimulatory molecules, an altered balance in IL-12p70 and IL-10 production and a poor capacity to stimulate T-cell proliferation and IFNγ production. Interestingly, upon cognate interaction with Th1 cells these tumor-induced M2macrophages could be switched to activated M1-like macrophages that expressed high levels of co-stimulatory molecules, produced high amounts of IL-12 and low amounts of IL-10, as well as acquired the lymphoid homing marker CCR7. The effects of the interaction between M2-macrophages and Th1 cells could partially be mimicked by activation of these APC via CD40 in the presence of IFNγ. Our data on the presence, induction and plasticity of tumor-induced tolerogenic APC in cervical cancer suggest that tumor-infiltrated Th1 cells can stimulate a tumor-rejecting environment by switching M2-macrophages to classical pro-inflammatory M1 macrophages. TUESDAY Designing T-cells with desired T-cell receptor make-up for adoptive immunotherapy M.M. van Loenen, R. de Boer, R.S. Hagedoorn, A.L. Amir, H.M. van Egmond, V. Jankipersadsing, J.H.F. Falkenburg, M.H.M. Heemskerk T-cell receptor (TCR) gene transfer is an attractive strategy to equip T-cells with defined antigen-specific TCRs using short-term in vitro procedures. Selection of host cells with a known specificity and introduction of a well characterized TCR may result in an off-the-shelf therapy that combines high anti-tumor reactivity with a minimal risk of off-target toxicity. For efficient anti-tumor reactivity, high expression of the introduced TCR is required. We have explored several strategies to optimize expression of the high affinity minor histocompatibility antigen specific HA-1-TCR and limit the expression of mixed TCR dimers, consisting of the endogenous TCR chains pairing with introduced TCR chains, that could harbor potentially harmful specificities. Of different strategies explored, the most marked improvement in HA-1-TCR expression and functionality was observed after TCR transfer of a cysteine modified and codon optimized HA-1TCR. Furthermore, results demonstrate that next to increased HA-1-specific reactivity, potentially harmful neoreactivities due to mixed dimer formation were dramatically reduced after cysteine modified HA-1-TCR gene transfer. To demonstrate the feasibility and study the efficacy of TCR gene transfer, we aim to start a clinical trial beginning 2012. In this trial, refractory leukemia patients that received allogeneic stem cell transplantation (SCT) will be treated with virus-specific donor T-cells engineered with the modified HA-1-TCR. To increase the number of patients that can be treated with TCR-modified T-cells, tumor associated antigens (TAA) are potential interesting target antigens. However, since most TAAs are self antigens, TCRs specific for TAAs presented in self-HLA are of low affinity. Recently, we isolated from a patient experiencing severe graft versus host disease (GvHD) after HLA-mismatched SCT several high avidity T-cells directed against TAAs presented in allo-HLA. These T-cells were demonstrated to exert single peptide specificity and recognition was strictly correlated with PRAME expression. However, next to high reactivity against multiple different PRAME positive melanoma and leukemic cells, limited on-target reactivity against matured dendritic cells and kidney epithelial cells was observed. Inclusion of a suicide gene as safety switch may be necessary to enable in vivo elimination of the engineered T-cells if adverse events occur. Human CD20 was proposed as a non-immunogenic suicide gene targeted by the widely used clinical-grade antibody rituximab and can additionally functions as a selection marker. However, transduction of T-cells with a bi-cistronic vector encoding both TCR and CD20 resulted in poor co-expression, due to unstable expression of CD20.don optimization of CD20 has recently demonstrated to allow high co-expression of both the PRAME-TCR and CD20. This co-expression allowed selection of engineered T-cells as well as efficient elimination of the cells in vitro. These results demonstrate that codon optimized CD20 can be a useful safety switch. TUESDAY Potent anti-tumor strategies based on OX40 engagement Daniel Hirschhorn Expansion and recruitment of CD4(+) Foxp3(+) regulatory T (T reg) cells are mechanisms used by growing tumors to evade immune elimination. In addition to expansion of effector T cells, successful therapeutic interventions may require reduction of T reg cells within the tumor microenvironment. We report that the combined use of the alkylating agent cyclophosphamide (CTX) and an agonist antibody targeting the co-stimulatory receptor OX40 (OX86) provides potent antitumor immunity capable of regressing established, poorly immunogenic B16 melanoma tumors. CTX administration resulted in tumor antigen release, which after OX86 treatment significantly enhanced the antitumor T cell response. We demonstrated that T reg cells are an important cellular target of the combination therapy. Paradoxically, the combination therapy led to an expansion of T reg cells in the periphery. In the tumor, however, the combination therapy induced a profound T reg cell depletion that was accompanied by an influx of effector CD8(+) T cells leading to a favorable T effector/T reg cell ratio. Closer examination revealed that diminished intratumoral T reg cell levels resulted from hyperactivation and T reg cellspecific apoptosis. Thus, we propose that CTX and OX40 engagement represents a novel and rational chemoimmunotherapy. TUESDAY Anti-CTLA-4 treatment in cancer James P. Allison and Padmanee Sharma Over the past several years it has become apparent that cell intrinsic and extrinsic regulatory pathways that act in concert to minimize harm to normal tissues have limited the effectiveness of active immunologic strategies for cancer therapy. We conducted extensive pre-clinical studies in mouse models which showed that blockade of the inhibitory signals mediated by CTLA-4 in T cells, either alone or in combination with a variety of immunologic and conventional therapies, led to tumor eradication and long-lived immunity. This work led to the generation of antibodies to human CTLA-4 and the conduct of an extensive series of clinical trials in human cancer. Over 6,000 patients have been treated with the CTLA-4 antibody Ipilimumab (Bristol-Meyers Squibb). Objective responses have been observed in metastatic melanoma, castrate resistant prostate cancer, as well as renal, lung, and ovarian cancer. In a recent Phase III trial, Ipilimumab was shown to prolong survival of stage IV metastatic melanoma patients, with 25% alive and ongoing at 4 years. This is the first drug of any type to show a survival benefit in metastatic melanoma in a placebo controlled randomized trial. In March 2011 Ipilimumab was approved by the FDA for both first and second line therapy of metastatic melanoma. A Phase III registration trial in castrate resistant prostate cancer is now underway. Recent studies have shown that the genetic instability inherent in cancer results in an extraordinary number of coding mutations in cancer. Many of these give rise to neoantigens which can provide multiple avenues for attack of tumor cells. It seems logical to begin to combine conventional therapies, or the new “targeted” therapies, that can cause tumor cell destruction with immune checkpoint blockade in order to obtain effective immune responses to these neoantigens, thereby effectively increasing the valency of therapy and minimizing the chances of acquistion of tumor resistance and escape. We have begun to explore the effects of targeted therapies on immune responses and whether the combination of anti-CTLA-4 and targeted therapy in pre-clinical models. The ultimate goal is to determine whether we can take advantage of the high response rate to genetically targeted agents with the durability of immunotherapy. WEDNESDAY Mechanisms of Protective Tumor Immunity Glenn Dranoff Efficacious cancer immunotherapies will likely require combinations of strategies that enhance tumor antigen presentation and antagonize negative immune regulatory circuits. We demonstrated that vaccination with irradiated, autologous melanoma cells engineered to secrete GM-CSF followed by antibody blockade of CTLA-4 accomplishes clinically significant tumor destruction with minimal toxicity in a majority of stage IV metastatic melanoma and some advanced ovarian carcinoma patients. The extent of tumor necrosis in post-treatment biopsies was linearly related to the natural logarithm of the ratio of infiltrating CD8+ effector T cells to FoxP3+ Tregs, suggesting that further Treg inhibition might increase the frequency of clinical responses. Through an analysis of cytokine deficient mice, we delineated a critical role for GM-CSF in Treg homeostasis. GM-CSF is required for the expression of the phosphatidylserine binding protein MFG-E8 in antigen presenting cells, whereas the uptake of apoptotic cells by phagocyte-derived MFG-E8 maintains peripheral Treg activity. The pharmacologic inhibition of MFG-E8 function through genetic or engineering-based approaches blocks Treg induction, which intensifies vaccineinduced responses, leading to the regression of established tumors in mice. The clinical translation of these therapeutic strategies to Phase I testing in humans is underway. The detailed analysis of patients achieving sustained clinical benefits from irradiated, autologous GM-CSF secreting tumor cell vaccines and CTLA-4 antibody blockade also affords a rich opportunity to identify antigens associated with immune-mediated tumor destruction and to delineate mechanisms of therapeutic immunity. We elucidated several of the molecular pathways that underlie these anti-tumor effects, including the NKG2D system and multiple secreted/or cell surface proteins that contribute to tumor promoting inflammation. The therapy-induced antibodies manifest functional activity in vitro, antagonizing tumor cell survival, invasive potential, and angiogenesis. These findings support a key role for humoral immunity in tumor destruction, and highlight interest in more detailed characterization of the anti-tumor B cell repertoire in vaccinated patients. WEDNESDAY The potency of human plasmacytoid dendritic cells to induce immune responses in melanoma patients Jurjen Tel, Daniel Benitez-Ribas, Erik Aarntzen, Gregor Winkels, Gerty Schreibelt, Cornelis J.A. Punt, Carl G. Figdor, I. Jolanda M. de Vries Plasmacytoid dendritic cells (pDCs) represent a highly specialized naturally occuring dendritic cell subset and are the main producers of type I interferons in response to viral infections. Combined with the capacity to mature and participate in the adaptive immune response this DC subset might represent a powerful candidate for DC-based immunotherapy. The clinical application of this specialized DC subset was long hampered by the lack of a clinical grade isolation procedure and an appropriate maturation stimulus. Here, we show the first phase I clinical trial using pDCs purified according to good manufacturing practice guidelines with the CliniMACS-based isolation procedure. In this clinical trial 5 stage IV melanoma patients received FSME-IMMUN® matured tumor peptide-loaded pDCs in escalating doses and were tested for vaccine related toxicity. Whereafter 10 more stage IV melanoma patients received tumor peptide-loaded pDCs. We characterized the immunological response induced by the pDCs in terms of FSME specific T-cell proliferation and antibody responses, and the decetion of tumor-peptide specific T-cells in blood and delayed type hypersensitiviy reactions. Moreover, we show the tracking of 111In-labeled pDC in vivo after vaccination and demonstrate that pDCs upon injection migrate to distant lymph nodes. In summary, mature tumor peptide-loaded pDCs were used, and tracked in vivo by 111 In labeling, in a clinical trial to induce antitumor responses in melanoma patients. WEDNESDAY Immune correlates of success and failure of therapeutic cancer vaccination. M.J.P. Welters, G.G. Kenter, C.J.M. Melief, S.H. van der Burg Persistent infection with oncogenic human papillomavirus type 16 (HPV16) results in anogenital lesions, such as vulvar intraepithelial neoplasia (VIN), and their subsequent progression to carcinoma. The development of HPV16-induced diseases is dependent on the oncoproteins E6/E7 and is associated with immune failure at three different levels. Patients either fail to induce an HPV16 E6/E7-specific response or mount a weak T-cell response. When present HPV-specific effector T cells may fail to infiltrate the lesions and last but not least the immune response can be suppressed at both the induction and effector level by HPV16 E6/E7-specific CD4+ regulatory Tcells. To overcome this immune deficit we have developed an immunotherapeutic vaccine strategy based on the use of synthetic long overlapping HPV16 E6/E7 peptides (HPV16-SLP). In a phase II clinical trial HPV16-SLP vaccination of patients with HPV16+ high-grade VIN lesions (VIN3) resulted in an objective clinical response rate of 79% and a complete and durable (>24 months) regression (CR) of the lesion in 47% of the patients. The clinical outcome was related to the size of the lesion at study entry. Examination of HPV16-specific immunity in relation to lesion size revealed that the patients with smaller lesions displayed much stronger vaccine-prompted HPV16-specific effector T-cell responses (already ex vivo detectable) with higher IFNγ (P=0.0003) and IL-5 (P<0.0001) levels than patients with large lesions. Characteristically, this response was accompanied by a distinct peak in cytokine levels after the first vaccination. Additionally, the group of CR patients harboured earlier and significant higher levels of HPV16 E6/E7-specific IgG levels as a result of a well induced Th2 response upon vaccination compared to patients with no CR (P<0.05). In contrast, the patient group with larger lesions displayed a weaker effector response and a stronger HPV16-specific regulatory immune response, as witnessed by a significantly lower IFNγ/IL-10 ratio and a significantly higher frequency of HPV16specific CD4+CD25+Foxp3-positive T cells (P=0.005) upon vaccination. In conclusion, the HPV16-SLP vaccine-induced immunity in patients, who were or were not successfully treated, revealed that therapeutic vaccination can be a truly effective therapy but it also teaches us that the HPV-specific CD4+CD25+Foxp3+ T cells expanded by vaccination mainly in patients with larger lesions at study entry can play a role in blunting vaccine-induced T-cell reactivity and clinical responses. Therefore, progressive disease may deregulate the specific immune response to such an extent that for those patients the current immunotherapy strategy needs further adjustment. WEDNESDAY Vaccination of melanoma patients with monocyte-derived dendritic cells matured with commonly used prophylactic vaccines Gerty Schreibelt, Erik Aarntzen, Kalijn Bol, Cornelis J.A. Punt, Carl G. Figdor, Gosse J. Adema, I. Jolanda M. de Vries Currently dendritic cell (DC)-based immunotherapy is explored in clinical trials, predominantly in cancer patients. Murine studies showed that only maturation with Toll like receptor (TLR) ligands generates mature DC that produce interleukin-12 and promote optimal T cell help. Unfortunately, the limited availability of clinical grade TLR ligands significantly hampers the translation of these findings into DC-based immunotherapy for cancer patients. We recently developed an alternative maturation cocktail containing the preventive vaccines BCG-SSI, Act-HIB and Typhim. This vaccine-cocktail contains TLR ligands and, when supplemented with prostaglandin E2, gives rise to highly mature, interleukin 12-producing DC that are able to migrate towards CCL21. In vitro, DC matured with the vaccine-cocktail are potent inducers of tumour antigen-specific T cells and Th1 polarization. We recently started a clinical trial in melanoma patients to investigate whether vaccine-matured DC improve antitumour responses in vivo. Thirteen patients were vaccinated intradermally and intravenously with increasing doses of DC. After vaccination, intradermally injected DC migrated to the lymph nodes and all patients developed a T cell response to the monitoring molecule KLH. However, the first clinical results suggest that toxicity is higher than after vaccination with DC matured with a cytokine cocktail (IL-1, TNF, IL-6, PGE2). Patients suffer grade I-II fever, fatigue, flu-like symptoms and injection site reactions. Some patients developed up to grade III liver toxicity and in two patients vaccine-specific T cells infiltrated in the lungs. However, these were temporary phenomena. Follow-up time is not sufficient to show whether the use of a vaccine-cocktail as maturation stimulus results in enhanced anti-tumour responses as compared to the cytokine cocktail. WEDNESDAY Plasmacytoid dendritic cells determine the in vivo function of specific subsets of conventional dendritic cells in tumor immunotherapy Nierkens S, den Brok MH, Garcia Z, Togher S, Wagenaars J, Boon L, Ruers TJ, Figdor CG, Schoenberger SP, Adema GJ,†, and Janssen EM. The differences in function, location and migratory pattern of conventional dendritic cells (cDCs) and plasmacytoid DCs (pDCs) may not only point to specialized roles in specific immune responses but also signify additive and interdependent relationships required to clear pathogens and boost immunity. Here we studied the in vivo requirement of cross-talk between cDCs and pDCs for eliciting anti-tumor immunity against in situ released tumor antigens in the absence or presence of the Toll-like receptor (TLR) 9 agonist CpG. Previous data indicated that CpG boosted tumorspecific T cell responses after in vivo tumor destruction and increased survival after tumor re-challenges. The present study shows that cDCs are indispensable for crosspresentation of tumor antigens released by ablation, while pDCs are essential to benefit from the immune stimulating effects of CpG. Depletion of pDCs inhibited CpG-stimulated priming of antigen-specific CD8+ T cells in blood, spleen and lymph nodes and significantly diminished the induction of long-term anti-tumor immunity. In the absence of pDCs, CD80 expression on cDCs was lower upon CpG administration. The efficacy of CpG was completely dependent on signaling through MyD88 and type I IFN. Moreover, by transferring wild type pDCs or cDCs into TLR9-deficient mice, we showed that TLR9 expression in pDCs is required to benefit from CpG as an adjuvant. Ex vivo characterization and DC-vaccination studies + revealed that CD11band the recently identified merocytic DCs were most + DCs were potent stimulators of CD8 T cells against antigens derived from dying cells, merocytic DCs strongly stimulated both CD4 and CD8 T cells. Hence merocytic DCs may be an even better target for DC + DCs. Fms-like tyrosine kinase 3 ligand (FLT3L) primarily expanded these specific subsets in vivo showing an association between the beneficial anti-tumor responses upon FLT3L treatment and the induction of merocytic DCs. These studies indicate that the efficacy of CpG to stimulate antitumor immunity is dependent on cross-talk between TLR9-expressing pDCs and specific subsets of cDCs. WEDNESDAY Coordinated isolation of CD8+ and CD4+ T cells recognizing a broad repertoire of cytomegalovirus pp65 and IE1 and adenovirus hexon epitopes for highly specific adoptive immunotherapy Maarten L. Zandvliet, Ellis van Liempt, Inge Jedema, Louise A. Veltrop-Duits, Henk-Jan Guchelaar, Arjan C. Lankester, Marco W. Schilham, J.H. Frederik Falkenburg, and Pauline Meij Adoptive transfer of specific cytomegalovirus (CMV)- and adenovirus (AdV)-specific memory T cells can be used for treatment viral complications after allogeneic stem cell transplantation (alloSCT). Since coordinated CD8+ and CD4+ T cells specific for a broad repertoire of viral-specific epitopes may be most effective for adoptive immunotherapy, the aim of this study was to isolate these cells from peripheral blood irrespective of the HLA type of the patient and donor. CMV pp65, CMV IE-1 and AdV hexon protein-spanning 15mer peptide pools were used to induce simultaneous activation of both CD8+ and CD4+ CMV-specific T cells. Isolation of IFNg-secreting cells resulted in efficient enrichment of CMV- and AdV-specific T cells. The T cell lines contained high frequencies of CD8+ and CD4+ T cells recognizing multiple CMV pp65, CMV IE1 and AdV epitopes. This study provides a feasible strategy for the rapid generation of clinical grade CD8+ and CD4+ T cell lines with high specificity for multiple CMV pp65, CMV IE1 and AdV hexon epitopes, and currently both methods are implemented into the clinic for the treatment of CMV or AdV induced complications after alloSCT. The generation of the CMV and AdV-specific T cell products has been translated to a clinical grade method, scaled up and validated. Furthermore specifications of the T cell products have been determined for the quality control and the release of the product before administration to the patient. WEDNESDAY Eradication of Human Papilloma Virus-induced tumors by combined treatment of low-dose chemotherapy and long peptide vaccination T.C. van der Sluis, S. van Duikeren, A. Sloots, F. Ossendorp, R. Arens, S.H. van der Burg and C.J.M. Melief. About 50% of the patients with Human Papilloma Virus (HPV) induced neoplasia display clinical benefit after treatment with Synthetic Long Peptide (SLP) vaccination. The success or failure of these vaccinations correlates clearly with the vaccineinduced T-cell immunity. Remarkably, some patients did not respond to vaccination until subsequent treatment with chemotherapeutic agents, suggesting that immunotherapy and chemotherapy may work synergistically. In a preclinical mouse model of HPV16-induced cervical cancer we tested experimentally whether chemotherapy could improve tumor eradication induced by a long peptide vaccine containing a cytotoxic T-cell epitope and a T-helper epitope. In most mice, peptide vaccination or a well tolerated dose of chemotherapy as a standalone therapy induced only a temporal decrease of the tumor size. Conversely, a combination of these therapies induced full tumor eradication in nearly all mice. Especially, the platinum anti-cancer drugs Cisplatin and Carboplatin work synergistically with SLP-vaccination. Importantly, tumor-specific T-cell responses appear not to be negatively effected by chemotherapy. Instead, the percentages of effector-memory like tumor-specific T cells are increased in mice receiving the combination therapy. The results of combination therapy with SLP vaccination and low dose chemotherapy have important implications for the rational design of the immunotherapy to cancer. WEDNESDAY Dissection of T cell therapy- and anti-CTLA4-induced cytotoxic T cell responses in melanoma Kvistborg P, Shu J, Heemskerk B, Thrue CA, Blank C, Besser M, Dudley ME, Hadrup S, Straten Pt, Haanen J, Schumacher T. There is strong evidence that melanoma-reactive T cell responses induced by immunotherapeutic interventions such as anti-CTLA4 (Ipilimumab) treatment or T cell therapy with tumor-infiltrating lymphocytes (TIL) can exert clinically meaningful effects. However, at present we have very little information on how these therapies influence tumor-specific T cell responses. Furthermore, as the number of potential melanoma-associated antigens to which these responses can be directed is very high, classical strategies to map cytotoxic T cell reactivity do not suffice. Knowledge of such reactivities would be useful to design more targeted strategies that selectively aim to induce immune reactivity against these antigens. In the past years we have aimed to address this issue by designing MHC class I molecules occupied with UV-sensitive ‘conditional’ peptide ligands, thereby allowing the production of very large collections of pMHC complexes for T cell detection. Secondly, we have developed a ‘combinatorial coding’ strategy that allows the parallel detection of dozens of different T cell populations within a single sample. The combined use of MHC ligand exchange and combinatorial coding allows the high-throughput dissection of diseaseand therapy-induced CTL immunity. We have now used this platform to monitor immune reactivity against a panel of over 200 melanoma-associated epitopes. Data on the composition of TIL products used for adoptive cell therapy and on the effect of TIL therapy or Ipilimumab treatment on the tumor-reactive T cell repertoire in melanoma patients will be presented. WEDNESDAY Idiotype Vaccination for indolent B-cell non-Hodgkin lymphomas Marcello Navarrete The clonal tumor immunoglobulin expressed on the surface of malignant B cells, termed idiotype (Id), has been used as a tumor-specific antigen in therapeutic vaccination strategies for indolent B-cell non-Hodgkin lymphomas. A number of phase 1 and phase 2 clinical trials have established the safety and immunogenicity of Id vaccination in follicular lymphoma (FL) and other indolent B-cell non-Hodgkin lymphomas. However, recently reported controlled randomized trials of idiotype vaccination for FL have yielded conflicting results. An improved understanding of the Id capable of acting as an antigen but also as an antigen receptor as well as a deeper insight into the mutual influences between the immune system and lymphoma are crucial for the future development of this non-toxic therapy. Id vaccination for follicular lymphoma was primarily being developed as remission consolidation after chemotherapy. We have recently reported data on Id vaccination as primary intervention for treatment-naive indolent B-cell lymphoma. Effective immunity against untreated lymphoma appears to be dependent on idiotype-specific T cells and sustained remissions in patients with vaccination-induced cellular immunity suggest clinical benefit. In addition, we have recently identified and characterized numerical and functional defects in circulating lymphocytes from patients with untreated chronic B-cell malignances in a prospective fashion. This data, together with the results of ongoing projects indicating that different modes of Id vaccination could differ in their propensity to generate the various T-cell subsets, may allow the development of strategies aimed for reprogramming the immune system from lymphoma-promoting effects toward adverse conditions for the malignant B cells. PARTICIPANTS Dr. James Allison Memorial Sloan-Kettering Cancer Center 1275 York Avenue Box 470, New York NY 10065 allisonj@mskcc.org Prof. Frances Balkwill Barts Cancer Institute Centre for Cancer and Inflammation London EC1M 6BQ United Kingdom f.balkwill@qmul.ac.uk Dr. Jasper van den Boorn Institut für Klinische Chemie und Pharmakologie Universitätsklinikum Bonn Sigmund‐Freud‐Str. 25 53127 Bonn Germany jvdboorn@uni-bonn.de Dr. Rinke Bos The Scripps Research Institute Dept. of Immunology/ Microbial Science 10550 North Torrey Pines Road La Jolla, CA 92037-1000 United States rinkebos@scripps.edu Prof. Vincenzo Bronte University Hospital Dept. of Pathology/Immunology Section P.le Aldo Scuro, 10, Verona (37134) Verona, Italy vincenzo.bronte@univr.it Prof. Günther Hartmann Institut für Klinische Chemie und Pharmakologie Universitätsklinikum Bonn Sigmund‐Freud‐Str. 25 53127 Bonn Germany gunther.hartmann@uni-bonn.de Dr. Thorbald van Hall LUMC Department of Clinical Oncology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands T.van_Hall@lumc.nl Dr. Ramon Arens LUMC Dept. of Immunotherapy and Blood Transfusion Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands R.Arens@lumc.nl Dr. Joost van den Berg Center for Cancer Immune Therapy (CCIT) University Hospital Herlev Herlev Ringvej 75 DK-2730 Copenhagen Denmark Jvan0008@heh.regionh.dk Prof. Maries van den Broek University Hospital Zurich Department of Oncology Rämistrasse 100/ Wagistrasse 14 8091 Zurich/ 8952 Schlieren Switzerland maries@van-den-broek.ch Claudia da Cunha Oliveira Msc LUMC Department of Clinical Oncology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands c.cunha-oliveira@lumc.nl Dr. Glenn Dranoff Dana-Farber Cancer Institute 450 Brookline Avenue, Dana 520C Boston, MA 02115 United States glenn_dranoff@dfci.harvard.edu Marieke Herbert-Fransen BSc LUMC Department of Immunotherapy and Blood Transfusion Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands M.F.Herbert-Fransen@lumc.nl Dr. Moniek Heusinkveld LUMC Department of Clinical Oncology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands m.heusinkveld@lumc.nl Daniel Hirschhorn-Cymerman Memorial Sloan-Kettering Cancer Center Tumor Immunology Laboratory 1275 York Avenue Box 470, New York NY 10065 hirschhd@mskcc.org Dr. Axel Hoos Bristol-Myers Squibb 5 Research Parkway Wallingford CT 06492 USA axel.hoos@bms.com Dr. Yvette van Kooyk VU University Medical Center Department MCBI Van der Boechorststraat 7 1081BT Amsterdam The Netherlands y.vankooyk@vumc.nl Dr. Thomas Kündig University Hospital Zürich Rämistrasse 100 8091 Zürich Switzerland Thomas.Kuendig@usz.ch Dr. Pia Kvistborg The Netherlands Cancer Institute Plesmanlaan 121 1066 CX Amsterdam The Netherlands p.kvistborg@nki.nl Dr. Marleen van Loenen LUMC Department of Hematology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands M.M.van_Loenen@lumc.nl Dr. Pauline Meij Dr. Carla Milagre Barts Cancer Institute Centre for Cancer and Inflammation Charterhouse Square London EC1M 6BQ United Kingdom c.s.milagre@qmul.ac.uk Dr. Marcelo Navarrete LUMC Department of Hematology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands m.a.navarrete@lumc.nl Prof. Sjaak Neefjes The Netherlands Cancer Institute Plesmanlaan 121 1066 CX Amsterdam The Netherlands Dr. Stefan Nierkens Nijmegen Centre for Molecular Life Sciences Department of Tumor Immunology Geert Grooteplein 28 6525 GA Nijmegen s.nierkens@ncmls.ru.nl j.neefjes@nki.nl Prof. Michel C. Nussenzweig The Rockefeller University Laboratory of Molecular Immunology 1230 York Avenue New York, NY 10065 United States nussen@mail.rockefeller.edu LUMC Dept. of Clinical Pharmacy/ Toxicology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands p.meij@lumc.nl Prof. Christian Ottensmeier Institute University of Southampton Somers Cancer Research Building MP 824, Tremona Road, Southampton SO16 6YD United Kingdom cho@soton.ac.uk Petra Paul MSc The Netherlands Cancer Institute Plesmanlaan 121 1066 CX Amsterdam The Netherlands p.paul@nki.nl Dr. Gertie Schreibelt Nijmegen Centre for Molecular Life Sciences Department of Tumor Immunology. Geert Grooteplein 28 6525 GA Nijmegen The Netherlands Rodney Rosalia MSc LUMC Department of Clinical Pharmacy and Toxicology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands r.a.rosalia@lumc.nl g.schreibelt@ncmls.ru.nl Dr. Pam Sharma MD Anderson Cancer Center 1515 Holcombe Boulevard Houston TX 77030 USA padsharma@mdanderson.org Prof. Linda Sherman The Scripps Research Institute Department of Immunology and Microbial Science 10550 North Torrey Pines Road La Jolla, CA 92037-1000 United States lsherman@scripps.edu Tetje van der Sluis MSc LUMC Department of Immunotherapy and Blood Transfusion Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands T.C.van_der_Sluis@lumc.nl Prof. Per Thor Straten Center for Cancer Immune Therapy (CCIT) Department of Hematology University Hospital Herlev Herlev Ringvej 75 DK-2730 Herlev, Denmark thorstraten01@heh.regionh.dk Dr. Wendy Unger VU University Medical Center Department MCBI Van der Boechorststraat 7 1081BT Amsterdam The Netherlands w.unger@vumc.nl Dr. Jolanda de Vries Nijmegen Centre for Molecular Life Sciences Department of Tumor Immunology Geert Grooteplein 28 6525 GA Nijmegen The Netherlands J.deVries@ncmls.ru.nl Dr. Marij J.P. Welters LUMC Department of Clinical Oncology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands m.j.p.schoenmakers-welters@lumc.nl Gijs Zom MSc LUMC Department of Immunotherapy and Blood Transfusion Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands G.G.P.Zom@lumc.nl ORGANIZING COMMITTEE Prof. Ferry Ossendorp LUMC Dept. of Immunotherapy and Blood Transfusion Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands F.A.Ossendorp@lumc.nl Dr. Sjoerd van der Burg LUMC Dept. of Clinical Oncology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands S.H.van_der_Burg@lumc.nl Prof. Wim Fibbe LUMC Dept. of Immunotherapy and Blood Transfusion Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands W.E.Fibbe@lumc.nl Prof. John Haanen LUMC Dept. of Clinical Oncology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands J.B.A.G.Haanen@lumc.nl Prof. Kees Melief LUMC Dept. of Immunotherapy and Blood Transfusion Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands C.Melief@lumc.nl Dr. Jaap Oostendorp Dr. Jaap Jan Zwaginga LUMC Dept. of Immunotherapy and Blood Transfusion Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands J.J.Zwaginga@lumc.nl LUMC Dept. of Clinical Pharmacy and Toxicology Albinusdreef 2, E3-Q 2333 ZA Leiden The Netherlands J.Oostendorp@lumc.nl