Clinical Decision Unit MULTIDISCIPLINARY CLERKING PROFORMA
Acute Anaphylaxis
Date & Time of arrival in ED
Patient ID details (include ED number)
Date & Time of arrival in CDU/OBS UNIT
Triage Category
Cubicle
Management
Inclusion criteria
(for CDU/OBS
UNIT)
Patients with acute allergy or anaphylaxis (<72 hours) that require a period
of observation after their initial treatment.
Patients must have all the following after their initial treatment:
Exclusion criteria
(any of)
SaO2 >95% on O2 or SaO2 >92% on air
Respiratory rate 10-20
HR 50-110
Systolic BP >100
GCS15
2 Intravenous access (one at least that is grey)
Patients that can be discharged directly from ED.
e.g. Patients with a non-progressing isolated allergic rash with no
systemic symptoms or signs and have not required parenteral
medication.
Necessity for more than a single dose of Adrenaline
Patients that require continuing resuscitation
Other coexisting acute condition requiring in-patient management
e.g. myocardial ischaemia
Initial assessment
Time
FiO2
(l/min or %)
Pulse
Blood
Pressure
RR
1
PEFR
(if appropriate)
O2 Sats
GCS
2
Summary of Acute Anaphylaxis Management Guideline
Management in ED
Management in
CDU/OBS UNIT:
Observations: temperature, pulse, blood pressure, respiratory rate, SaO2, PEFR
(if bronchospasm), GCS,
Treatment:
Resuscitation
Intravenous access
Adrenaline IM (IV)/ Chlorphenamine/ Steroids -as appropriate
Nebulised bronchodilators if significant wheeze
Consider H2 Blockade for resistant urticaria
Patient must remain in ED for at least 2 hrs to confirm clinically
stable prior to transfer to CDU
Investigations:
FBC, U&E, RBS
Mast Cell Tryptase
Observations: Continuous ECG and SaO2 monitoring
Every 30 mins the patients general clinical status should be assessed along with
the following observations: Airway assessment
Pulse, Blood pressure,
Respiratory Rate,
PEFR (if bronchospasm)
Treatment:
Oxygen to keep SaO2 > 95%,
Chlorphenamine 4mg tds (safe in pregnancy)
Prednisolone 40mg od for 2-3 days
Salbutamol 5mg neb for bronchospasm
Timing of review
If clinical deterioration- at any time
If isolated urticaria - 2 hours
All other patients - 6 hours
Consider more prolonged observation (8-24hours) for:
Severe reactions with slow onset
Reactions in severe asthmatics or with a severe bronchospasm
Reactions with the possibility of continuing absorption of allergen
Patients with a previous history of biphasic reactions
Criteria for discharge
(All must be met)
Criteria for admission
(at any time)
Indications for Epipen
The patient must have normal physiology
Symptoms and signs must be resolved or if still present have
progressively improved during the observation period
GP letter sent
Discharge medication as above. (See indications for Epipen)
Verbal and written discharge advice
Referral for investigation (by GP) suggested on discharge letter
Unstable patient requiring resuscitation of ABC'S
Social circumstances prevent discharge
Sudden onset life threatening reaction to unknown / unavoidable
substance.
High likelihood of recurrence
3
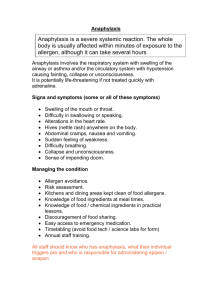
Emergency Management of Anaphylactic Reaction
(From Resus Council(UK))
Airway, Breathing, Circulation, Disability, Exposure,
Diagnosis - look for:
• Acute onset of illness
• Life-threatening Airway and/or Breathing
and/or Circulation problems1
• And usually skin changes
• Call for help
• Lie patient flat
• Raise patient’s
legs
Adrenaline2
When skills and equipment available:
• Establish airway
• High flow oxygen
Monitor:
• IV fluid challenge 3
• Pulse oximetry
4
• Chlorphenamine
• ECG
5
• Hydrocortisone
• Blood pressure
1 Life-threatening problems:
Airway: swelling, hoarseness, stridor
Breathing: rapid breathing, wheeze, fatigue, cyanosis, SpO2 < 92%, confusion
Circulation: pale, clammy, low blood pressure, faintness, drowsy/coma
2 Adrenaline (give IM unless experienced with IV adrenaline)
IM doses of 1:1000 adrenaline (repeat after 5 min if no better)
• Adult
• Child more than 12 years:
• Child 6 -12 years:
• Child less than 6 years:
500 micrograms IM (0.5 mL)
500 micrograms IM (0.5 mL)
300 micrograms IM (0.3 mL)
150 micrograms IM (0.15 mL)
3 IV fluid challenge:
Adult 500 – 1000 mL
Child crystalloid 20mL/kg
Stop IV colloid
if this might be the cause
of anaphylaxis
Adrenaline IV to be given only by experienced specialists
Titrate: Adults 50 micrograms; Children 1 microgram/kg
4 Chlorphenamine
(IM or slow IV)
Adult or child more than 12 years
Child 6 - 12 years
Child 6 months to 6 years
Child less than 6 months
10 mg
5 mg
2.5 mg
250 micrograms/kg
4
5 Hydrocortisone
(IM or slow IV)
200 mg
100 mg
50 mg
25 mg
Medical Notes
History presenting complaint
Past Medical History
Drug History
Examination findings
Management:
1.
2.
3.
4.
Impression/Diagnosis
Signature
Date
Print Name
Time
5
Investigations Requests
The following investigations may be performed on all those with acute allergy / anaphylaxis
Investigation
When performed
Dr/Nurse
Time
signature
Reason if not performed
ECG
CXR
Arterial blood
gases
FBC, U&E, glucose
Mast Cell
Tryptase
Investigation results
Result
Signature Date/Time
Hb
ECG
WCC
Platelets
Na
K
Chest X-ray
Urea
Creatinine
FiO2
SaO2
Other investigations
PH
PO2
PCO2
Mast Cell
Tryptase
6
Free text page (for use by all staff on CDU)
Date and Time
Comments / notes
Signature
7
Free text page (for use by all staff on CDU)
Date and Time
Comments / notes
Signature
8
CLINICAL DECISION UNIT DISCHARGE SUMMARY
Anaphylaxis
PATIENT NAME/
ADDRESSOGRAPH
GP Details:
Name
Address
ADDRESS
DATE OF BIRTH
Dear Dr
Your patient attended the Clinical Decision Unit at Huddersfield Royal Infirmary with
ANAPHYLAXIS / MODERATE ALLERGIC REACTION(delete as appropriate)
The precipitant appeared to be
Your Patient DID / DID NOT require Adrenaline to control their symptoms.
□ Your patient has been advised to contact yourself or the Emergency Department at Huddersfield
Royal Infirmary should there be any further problems.
□ Your patient has been advised to contact yourself with a view to consideration of further
investigation by an Immunologist
Additional Comments
Thank You
Signed
Name
Designation
Date ________________
9
 0
0