EMORY GENETICS LABORATORY TEST REQUISITION FORM
advertisement

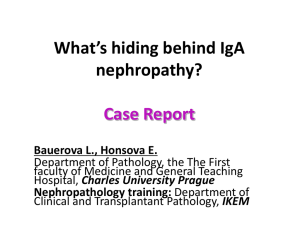
EMORY GENETICS LABORATORY TEST REQUISITION FORM - Page 1 of 1 2165 N. Decatur Rd., Atlanta, GA. 30033 ▪ (404)778-8500 or 1-800-366-1502 ▪ FAX (404) 778-8559 ▪ www.genetics.emory.edu PATIENT INFORMATION: SPECIMEN INFORMATION: Last Name __________________First_____________________MI_______ Date Collected_______/_______/_______Time_______:_______AM/PM Parents Names (if pt is a minor)____________________________________ SAMPLE TYPE: DOB______/________/________ Gender: Male Female Unknown __ Blood(B) _X__ Saliva Sample _____Other ___________________________ Mailing Address________________________________________________ City______________________________State_______Zip______________ Preferred Phone# (_________)___________-________________________ REASONS FOR REFERRAL: (check all that apply) Is this #: Home _X__Family history of __Fabry Disease_(272.7) ___ Other ____________________________ Work Cell Other: ____________________________ Other # where pt. can be reached: ( Ethnicity of Pt. (circle all that apply): Caucasian/NW European Jewish-Ashkenazi Native American Other ) - . African-American Asian East Indian Hispanic Jewish-Sephardic Mediterranean Native Hawaiian/Other Pacific Islander PREVIOUS LAB RESULTS: See attached report with identified family mutation SPECIAL INSTRUCTIONS: Fabry Family Member Testing project (AAKP) PHYSICIAN ORDERING TEST: Paperwork to be reviewed by genetic counselor Name________________________________________________________ [ ] Please mark this box if you do NOT want to be contacted about future Fabry related research studies. Practice Name_________________________________________________ Address______________________________________________________ City______________________________State_______Zip______________ BILLING INFORMATION: Preferred Phone# (_________)___________-________________________ Fabry Family Member Testing project, bill to American Association of Kidney Patients (client number 4926) FAX# (__________)____________________________________________ Genetic Counselor_______________________Phone__________________ Molecular Test DUPLICATE REPORTS TO: Name____Dawn Laney, MS, CGC_______________________________ _________ Address__Emory LSDC, 2165 North Decatur Road______________ City_____Decatur___________State__GA___Zip___30033____ Preferred Phone# (_404__)___778___-___8518__________ FAX# (__404__)___778-8562______________________________ Rec/d____/____/0__ Unboxed by________________Sender:______________________ TEMP SPECIMEN COLOR #TUBES COMPLETE R C F PT. DATA R C F TEST DATA R CF LABELS THIS BOX FOR LAB USE ONLY INC NOTES: Fabry Family Member Testing (KM): Targeted mutation testing for previously identified family mutations. (A report of the family mutation must accompany submitted sample)






![[Date] - Fabrazyme](http://s3.studylib.net/store/data/007856986_2-92736280fd31154fb73068d0df9b074f-300x300.png)