Medical Mycology (BIOL 4849) Summer 2007
advertisement
 Summer 2007")
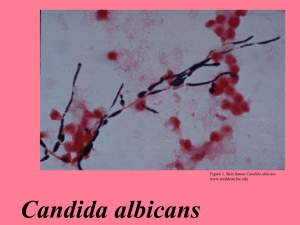
Medical Mycology (BIOL 4849) Dr. Cooper Summer 2007 Candidiasis Synonyms: candidosis, candidal infection, candidemia, candidiasis syndromes Candidiasis •primary or secondary myotic infection caused by members of the genus Candida •opportunistic pathogens •produce a wide spectrum of diseases •Most common cause of fungal infection affecting immunocompromised patients Presentation of Disease creamy, white, thick patches on mucosal surfaces consists of moist rashes with lesions surrounding skin Case Report 1 Can J Ophthalmol (2007) 42: 154-155 •74-year-old man developed anterior uveitis 3 weeks after eye cataract surgery which is an inflammation of the middle of the eye -treatment was done with antibiotics, steroids, and soon after chemotherapy was started -the infection went away, but soon after there was recurrence of the disease -a sample from the inflamed part of the eye was examined and grown in agar -the agar chamber grew Candida albicans endophthalmitis, which simply put is a fungal infection in the eye •Candida endophthalmitis is rare and shows up many weeks after surgery -there is minimal pain, relatively good vision. -treatment can be done with fluconazole, amphotericin B and many other systemic antifungal preparations. -recurrence occurred because antifungal treatments were not used the first time to treat the patient Case Report 2 The Japanese Society of Internal Medicine. DOI: 10.2169/internalmedicine.45.1761 (PubMed, May 27, 2008). Candida albicans Endophthalmitis after Extracorporeal Shock Wave Lithotripsy in a Patient with Liver Cirrhosis ( Nabuyuki Toshikuni, Kazuhiro Ujike, Toshihiro Yanagawa, et al.): – March 2005, 69 year old male with left ureteral stone – ESWL uses shock waves to break a kidney stone into small pieces that can more easily travel through the urinary tract and pass from the body. – One day later the patient felt fatigue, and 3 days later liver function deteriorated. – The diagnosis of urinary tract infection and fungemia due to Candida albicans associated with decompensated liver cirrhosis and renal failure was made – Developed because of hepatic failure after extracorporeal shock wave lithotripsy during hospitalization. Cadida albicans: – is among the gut flora, the many organisms which live in the human mouth and gastrointestinal tract. – Under normal circumstances, C. albicans lives in 80% of the human population with no harmful effects. However, overgrowth results in candidiasis especially in immunocompromised patients. Treatment – Voriconazole and lipsomal amphotericin B, antifngal agents with strong activity against a broad spectrum of fungi were used – Patient was discharged in 61 days, however in November 2005, patient relapsed with poor visual acuity. – Surgery corrected endophthamitis of left eye – As of July 2006, patient has not relapsed Case Report 3 The Japanese Society of Internal Medicine. DOI: 10.2169/internalmedicine.46.6354 (PubMed, May 27, 2008). Dengue Fever/Dengue Hemorrhagic Fever (Satoshi Suzuki, Takatoshi Kitazawa, Yasuo Ota, et al.): –Acute fever causing disease often found in the tropics or in Africa. –Brought on by the bite of a mosquito (similar to malaria). –Symptoms most commonly seen are: fever, rash, mild liver dysfunction and complications can progress to liver failure and encephalopathy. –G.I. tract candidiasis, are problems associated with esophagitis due to herpes simplex, herpes zoster, induced by radiation, or gastroesphopaheal reflux disease. –Genitourinary tract candidiasis, are problems associated with bacterial cystitis or pyelonephritis. –Never been jointly associated together with Dengue fever. Patient is a 50 y o. asian male. • Initial cc was prolonged fever (39 C) with skin rash. • No significant social or sexual hx, no prior medical hx, or family hx relating to disease. • Travel to hx Sri Lanka for work in past 2 years, which is where he may have acquired the • disease. (August 25th) Pt. presented w/ prolonged fever 39 C. • Had normal, non-remarkable laboratory labs with noted slightly high platelet counts and • elevated liver enzymes. Enzyme-Linked Immunosorbent Assay (ELISA) showed IgM antibody for Dengue virus. • Polymerase Chain Reaction (PCR) assay confirmed Dengue viral RNA. • (August 26th) Pt. platelet counts dropped by factor of four and was given a platelet • transfusion. Pt. systolic b.p. dropped below 60mmHg and hematocrit was increased by 53.2% • Histopathology •Various Species of Candida: –C. Cutaneous (skin) –C. Mucocutaneous (mucus membrane) –C. Esophagitis (throat) –C. Onychomycosis (nails) –C. Oropharyngeal (mouth) –C. Vulvovaginitis (vagina) –C. Endophthalmitis (eye) Clinical Manifestations •Vulvovaginitis– Recurrent episodes of Candida vaginitis associated with the classic symptoms of pruritus, burning and abnormal discharge •Oropharyngeal-sore •Gastrointestinal•Respiratory •Central and painful mouth, burning mouth and tongue Heartburn, bloating, diarrhea, or constipation allergy- Rhinitis, sneezing, and wheezing Nervous System- Anxiety, depression, memory deficits, and loss of ability to concentrate •Other Systemic Symptoms- Fatigue, headache, irritability, Nausea, and vomiting, abdominal pain, fever, chills Laboratory Aspects Virulence Factors: •Surface molecules that permit adherence of the organism to other structures such as human cells, extracellular matrix, and prosthetic devices Diagnosis: •Diagnosis requires clinical, epidemiological, and laboratory findings •Positive culture growth of Candida from sterile specimens Epidemiology and Ecology •Ecology - found in soil, inanimate objects, food, hospital environments •Epidemiology - use of broad spectrum antibiotics - use of oral contraceptives - diets rich in yeast and carbohydrates - pregnancy - advanced surgical techniques Treatment and Prevention Treatment •Long-term therapy with antifungal agents at increasing doses until resolution of symptoms. Oral and usually vaginal nystatin are recommended. Other azoles, suck as ketoconazole have been also used. •Diet modification including restriction of sugar and other simple carbohydrates Prevention •Candida allergy shots •Avoidance of moldy environments References • “Candidiasis: Overview and Full Index” http://doctorfungus.or/mycosies/human candida/Chronic_Cand.. Article acquired May 27, 2008 from Doctor fungus. • “Chronic Candidiasis.” May 27, 2008. http://doctorfungus.or/mycosies/human candida/Chronic_Cand.. Article acquired May 27, 2008 from Doctor fungus. • Ellis, David. “Candidiasis.” The University of Adelaide. Mycology Online. 2006. http://www.mycology.adelaide.edu.au/Mycoses/Cutaneous/ Candidiasis/ Article acquired May 27, 2008. • Hildago, Jose A., Vazquez, Jose A., Shepp, David, et al. “Candidiasis.” December 15, 2005. http://www.emedicine.com/med/TOPIC264.HTM Article acquired May 27, 2008 from PubMed. • Suzuki, Satoshi, Kitazawa, Takazawa, Ota, Yasuo, et al. “Dengue Hemorrhagic Shock and Disseminated Candidiasis” The JapaneseSociety of Internal Medicine. 2007. DOI: 10.2169/internalmedicine.46.6354 http://www.naika.or.jp/imindex.html Article acquired May 27, 2008 from PubMed. • Toshikuni, Nobuyuki, Ujike, Kazuhiro, Yanagawa, Toshihiro, et al. “Candida Albican Endopthalmitis After Extracorporeal Shock Wave Litotripsy In a Patient With Liver Cirrhosis.” The Japanese Society of Internal Medicine. 2007. DOI: 10.2169/internal medicine.45.1761 http://www.naika.or.jp/imindex.html Article acquired May 27, 2008 from PubMed. • Weinstein, Orly, Levy, Jaime, and Lifshitz. “Recurrent Candida Albicans Endopthalmitis In An Immunocompromised Host.” Can J. Opthalmol. 2007; 42:154-5. Article acquired May 27, 2008 from PubMed.