Dear Notetaker:

BHS 116.1 – Human Physiology and Pathology
Notetaker: Emily Sorenson
Date: 09/30/11, 2 nd hour
Page1
AIMS:
Ventilation (cont.)
Diffusion of O
2
and CO
2
Between alveoli and blood
Topics
Pulmonary (minute) Ventilation o The total amount of new air moved into the respiratory passage each minute
Includes mouth, nasal passage, bronchi, trachea, alveoli o Tidal volume (air brought in) X respiratory rate (12 breaths per min) = 6 L/min
Rate can be altered: can get up to 40-50 breathes/min
Tidal volume can change: up to 4500 mL o Pulmonary ventilation: 150-200 L/min - can get very HIGH
Max respiratory rate and tidal volume
Can only sustain this for a short time – until physical exhaustion
Anatomic Dead Space o Alveoli is the only place where air is exchanged with blood o Tidal volume includes air in mouth, nasal passage, trachea, bronchi, etc.
This is the anatomic dead space because there is no exchange occurring here
About 150 mL o Only 350 mL of new air will actually reach the alveoli with each breath
150mL of total 500mL expired is old air
Comes from anatomic dead space of last breath o Expiration pushes out 500 mL at same time L: 350 (new air) + 150 (old air)
Alveolar Ventilation o Total amount of NEW air that reaches the alveoli / min o Equals : respiration rate X ( tidal volume – dead space volume ) o In normal situation: = 4.2L /min o 1.8 L less than the total amount of air brought in during pulmonary ventilation o Key: this is the new air that gets to alveoli vs. total amount we actually bring in
Respiration o Respiratory rate can change o Tidal volume can change o Dead space volume never changes = always 150 mL
BHS 116.1 – Human Physiology and Pathology
Notetaker: Emily Sorenson
Date: 09/30/11, 2 nd hour
Page2 o Normal Pulmonary ventilation: 6 L / min o Normal alveolar ventilation: 4.2 L / min o During deep, slow breathing
take in 1200 mL/breathe, but takes longer - so less breaths/min
increases tidal volume
decreased respiratory rate
Dead space and pulmonary ventilation don’t change
Since tidal volume has increased, will have a higher alveolar ventilation
More air brought into alveoli during deep slow breathing
More O
2
into system
Easily exchangeable with blood o Rapid, shallow breathing (hyperventilation)
Respiratory rates = 40 breathes / min but only 150 mL / breathe
Tidal volume = dead space volume 0 mL/min ventilation
No new air is getting into lungs (alveoli)
No O
2
/CO
2
exchange in blood
NOTE: Residual volume: still air in the lungs and capability of exchange with blood, but will be used quickly if no new air is being delivered
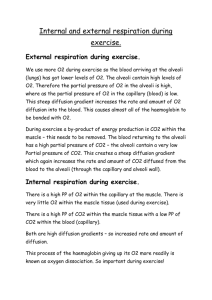
Diffusion of O
2
and CO
2
between Alveoli and Blood o Respiratory passage, functional part of lung = alveoli
Exchange occurs with blood vessels
O
2
goes from blood to the alveoli
CO
2
goes from the alveoli to the blood
Diffusion (simple) o Occurs down concentration gradient
Gas Pressure/ Partial Pressures o Partial pressure is proportional to (gas molecules) o Air is made up of many different gasses
Total atmospheric pressure: 760 mmHg
79% N
BHS 116.1 – Human Physiology and Pathology
Notetaker: Emily Sorenson
Date: 09/30/11, 2 nd hour
Page3
21 % O – Partial Pressure (pp): 160 mmHg o Partial pressure: fractional amount of the given gas in the total amount of air/atmosphere
(in terms of pressure) o Gas has to diffuse into liquid (blood) : so pp will play a different role when we discuss diffusing a gas into the liquid
Henry’s Law o Partial pressure = concentration of dissolved gas solubility (diffusion) coefficient
Gas has to be soluble in the liquid o Higher solubility coefficient = less pp required to dissolve specific gas into liquid o Low solubility Coefficient = more pp required to dissolve specific gas into liquid o CO
2
can dissolve in the blood at much lower partial pressure than O
2
Need higher pp of O
2
to dissolve the same amount of particles in the liquid
Net Rate of Diffusion of Gasses in Fluids o Fick’s Law
Looks at diffusion rate
gasses diffuse in and out of blood at different rates
there are many factors that play a role in determining a diffusion rate into gas
change in pressure: ions or gasses travel down gradient
cross sectional area: greater cross sectional area = greater diffusion rate o depends on size of alveoli or blood vessel
solubility: More soluble gas will diffuse faster : CO2 faster than O2
Distance of diffusion: how far does it have to diffuse o Distance: normally doesn’t play a role, but with pathological systems, the distance might increase, making it harder to diffuse
Size: larger molecules = slower diffusion
Alveolar Air o Air comprised of : N, O, AND small amounts of CO
2
and H
2
O o Air moves from atmosphere through respiratory passage into alveoli o In transit, from atmos. to alveoli, air will get humidified through trachea and bronchi
now water has larger component
pp O
2
will drop (to about 100 mmHg)
BHS 116.1 – Human Physiology and Pathology
Notetaker: Emily Sorenson
Date: 09/30/11, 2 nd hour
Page4
Due to fact that it is getting humidified and that the alveoli is constantly exchanging with the blood, (O
2
molecules are leaving, pp decreases)
CO
2
is also much higher in the alveoli (140mmHg) because the blood is constantly bringing it to the alveoli
Difference between the pp of atmospheric air that we bring in to the pp that are observed in the air in the alveoli
Alveolar Air Replacement Rate o 2700 mL of air in lungs after tidal volume is taken in o Of that, only 350mL is new (1/7 – 1/8 th of total amt of air is replaced during each breath)
Prevents sudden changes in blood gas concentrations (partial pressures)
Partial Pressure Changes Across Respiratory & Systematic Membranes o O
2
diffuses from the lungs (alveolar system) into pulmonary capillaries and then out of systemic tissue capillaries into tissues: downward diffusion
O
2
diffuses out of lungs into tissues o CO
2
diffuses out of tissues at systesmic capillaries, carried through venous system, leaves pulmonary capillaries into alveoli
CO
2
out of tissues into alveoli (lungs) o Partial Pressures driving exchange
pp O
2
in alveoli is 100mmHg
pp O
2
in tissues is 40mmHg (because being used in tissues for metabolism)
pp CO
2
of in alveoli is 40mmHg
pp CO
2
in tissues is 46mmHg (because this is being produced via metabolism) o Blood equilibrates to whichever region it is located
Arteriole blood: pp O
2
=100mmHg; pp CO
2
=40mmHg
Venous blood: pp O
2
=40mmHg; pp CO
2
= 46mmHg
Respiratory Unit o Alveoli and the pulmonary capillaries = where exchange is occurring in the lung
BHS 116.1 – Human Physiology and Pathology
Notetaker: Emily Sorenson
Date: 09/30/11, 2 nd hour
Page5
Respiratory Membrane o Consists of all the cell membranes and other components lining the respiratory units
alveolar cell membranes, capillary epithelial cell membranes, Surfactant, water, interstitial tissue/fluid o Total distance = 0.5 µ m o Alveoli and capillary are very close but there is some interstitial space between them o Main components making up membrane
Pulmonary capillary alveolar fluid
Type 1 alveolar cell
Cells of the Alveoli o Type 1: primary alveolar cell, lines the alveoli
Equivalent of endothelial cell lining the capillary
1 cell thick o Type 2 : produce and secrete surfactant
Release into alveoli o Type 3: macrophages
Aka: Dust cell
Phagocytes that take up dust particles, virus, bacteria, etc
Gas Diffusion Through Respiratory Membrane o 6 layers O
2
diffuses through:
Fluid and surfactants
Alveolar epithelium: Type I
Alveolar epithelial basement membrane
Interstitial space: this is very small (this is where problems occur in pathology)
Capillary endothelial cell basement membrane
Capillary endothelial cells
Factors affecting the rate of gas diffusion through the respiratory membrane o Can see changes with:
Surface area, thickness of membrane, and pp changes o Thickness of respiratory membrane (6 layers)
rarely changes - only during pathological changes o Surface area – can have expanded alveoli or blood vessels could diffusion rate o Diffusion coefficients of gasses (doesn’t change)
BHS 116.1 – Human Physiology and Pathology
Notetaker: Emily Sorenson
Date: 09/30/11, 2 nd hour
Page6 o Primary factor: Partial pressure difference between the blood and alveoli
Chart explains how certain changes affect the diffusion at respiratory membrane
Under constant resting conditions: we don’t usually see this changes, but
Diffusion Capacity of the Membrane o Volume of gas that will diffuse through it per minute (based on 1 mmHg change)
we do see them during exercise:
Under exercise: o Bring more air in o Expanding alveoli o Delivering more blood to lungs o Blood vessels increase in diameter o Increase surface area of respiratory membrane o Diffusion is easier for O
2
and CO
2
Above conditions decrease with pathological circumstances
During Exercise the Diffusion Capacity Changes due to: o Looking at the affects of normal diffusion capacity of O
2
and CO
2
Normal:
CO
2
: 20 fold greater diffusion capacity because its diffusion coefficient is greater
**always easier for CO
2
to diffuse than O
2
Exercise
Diffusion capacity of both increase sufficiently
Due to increase in surface area of respiratory membrane
Capillaries open up (that weren’t open prior)
Alveoli expand because we are bringing more air in
BOTH of these together increase the diffusion capacity of O
2
Ventilation-Perfusion Ratio (VP ratio) o Ventilation: brings air into alveoli o Perfusion: blood flow to alveoli o Zero ratio if we don’t have any ventilation (no air brought in)
BHS 116.1 – Human Physiology and Pathology
Notetaker: Emily Sorenson
Date: 09/30/11, 2 nd hour
Page7 o Infinity ratio if we don’t have any blood flow o During either of these cases, there is NO gas exchange
Either shut off O
2 delivery or blood flow o Physiological shunts
VP ratio is less than normal
Due primarily to decreased ventilation
Blood flow is typically normal or increased to the area
ventilation decreases and doesn’t match the blood flow
Blood flows through but no O
2
exchange
Effects:
Alveolar pp O
2
will be less than 100 mmHg
not bringing in enough fresh air (ventilation decreased)
Blood pulls it out, but alveoli isn’t delivering
pp CO
2
will be more than 40mmHg , because blood keeps delivering
CO
2
to the alveoli, but it isn’t getting expired as frequently o Physiological dead space
Plenty ventilation but decreased blood flow to that area
O
2
cannot be given up into blood and thus not delivered to tissues
Effects:
Bring in plenty of O
2
so pp O
2
is greater or equal to 100mmHg
No blood flow to pull O
2
away at the normal rate
O
2
will build
CO
2
is less than 40mmHg because no blood brings the CO
2
there o Graphically (lecture 25, pg 7):
Black line: VP ratio
X axis: sections of the lung: top to bottom (L-R)
Top of lung = dead space, air gets in no problem but blood flow is much lower than at the bottom
The top of the lung is above the heart; heart must pump harder to get it
UP to the top of the lung
BHS 116.1 – Human Physiology and Pathology
Notetaker: Emily Sorenson
Date: 09/30/11, 2 nd hour
Page8
Greater ventilation than Perfusion at top of lung, creates the dead space
Higher pp O
2
and Lower pp CO
2
Bottom of the lung = (opposite: physiologic shunt)
Less air relative to perfusion
Bottom of lung is right next to heart high perfusion levels of blood
Air flow is a lot lower than perfusion: no match of blood flow to air flow
Alveolar pp O
2
less than 100mmHg, pp CO
2
are much higher than
40mmHg o Lung Picture (Lecture 25, pg 7)
Upper lung :
VP ratio high (dead space in this area)
Lower blood flow compared to ventilation
Bottom Lung:
Low VP ratio
Greater blood flow than air flow
When we exercise:
Dilate blood vessels
More blood to lungs
More air intake into lungs
Normalizes both areas to normal VP ratio of 1 : better match of blood flow to air flow during exercise o Helps to normalize top and bottom portions of lung o Better 0
2
delivery and CO
2
expiration during exercise o Entire lung is under normal VP ratio, rather than just the middle
Local Controls of Ventilation-Perfusion Ratio o Local Controls
Physiological shunt:
High profusion, Low ventilation
Smooth muscle of arteriole and bronchioles will help to equalize 2 factors: o Increase CO
2
in alveoli = causes relaxation of bronchiolar smooth muscle
BHS 116.1 – Human Physiology and Pathology
Notetaker: Emily Sorenson
Date: 09/30/11, 2 nd hour
Page9
Dilate airways : Increases air flow o Decreased O
2
in alveoli = causes contraction of pulmonary arteriolar smooth muscle
Blood flow decreases
Air flow increases
Dead space
Lots of airflow, little blood flow o Decrease in CO
2
= causes contraction of bronchiolar smooth muscles
Constriction of airways, increased resistance, decreased air flow o Increase in O
2
= Causes dilation of local arterioles
Increase in blood flow to the area o Body has normal regulatory controls based on O
2
and CO
2 concentration affecting bronchiolar and pulmonary arteriolar smooth muscle
Q: When is pulmonary ventilation equal to alveolar ventilation?
1.
When tidal volume inc
2.
When tidal volume decrease
3.
When respiratory rate is increased
4.
When respiratory rate is decreased
5.
Never **CORRECT: we always have dead space. They can NEVER be equal. There will always be regions where they are equal with the blood.