Patho Review 7
advertisement

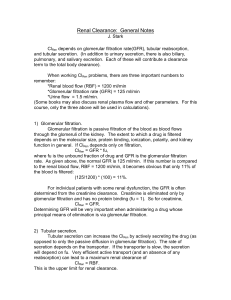
Patho Review 7 Introductory Concepts 1. At rest, about 20-25% of the cardiac output passes through the kidney. About 1/10 of this amount is filtered in the glomerulus to become an ultrafiltrate of plasma which subsequently passes through the renal tubular system. Blood flow to the kidney: • Rate of blood flow = 1~1.5 L/min • Blood volume filtered = 180 L/day 2. The kidney is composed of high pressure capillary filtration system (glomerulus) and low pressure capillary reabsorption system (peritubular capillaries) that surround the tubules. 3. The glomeruli of the kidney are actually extensions of the body's capillary system and the filtration of fluid from the glomerulus into Bowman's capsule is regulated by the same forces that affect capillary fluid exchange in other parts of the body; namely mechanical pressure and osmotic pressure. The glomerular filtration rate (GFR) is 125ml/min, or 180 L/day Under many condition, the plasma level of creatinine is a relatively good index of GFR. GFR = Cinulin ≈ Ccreatinine 4. While the glomeruli filter the blood, the renal tubular structures are responsible for the reabsorption of organic and inorganic materials needed to maintain the constancy of the internal environment. 5. Renal Functions: A) Urine formation - Urea; BUN 8-28 mg/ml (25-30g. produced daily) B) Elimination of waste products 1) Uric acid (normal value 3.0 to 5.0 mg/ml) 2) Creatinine ; 0.5-1 mg/ml (1-2g. produced daily) 3) Others – (Sulfates, Nitrates, Phosphates, Magnesium) C) Regulating hormones and enzymes Erythropoietin • Endothelial cells of peritubular capillaries secrete erythropoietin in response to hypoxia for RBC formation --- Anemia of Chronic Renal Failure (body cannot create enough EPO) Vitamin D Metabolism • Conversion of 25-OH vitamin D (storage form) to 1,25-(OH)2 vitamin D (active form) by 1α-hydroxylase, which is activated by PTH. Renin • JG cells secrete renin in response to ↓ renal arterial pressure and ↑ renal sympathetic discharge (β1 effect) --- Renin-Angiotensin-Aldosterone System Prostaglandins • Secretion of prostaglandins that vasodilates the afferent arterioles to increase GFR. D) Homeostatic regulation: 1) ECF volume and osmolarity (ADH) - The kidney regulates blood pressure through changes in blood volume (Na & H2O changes through the renin-angiotensin aldosterone mechanism and ADH. 2) Na+ retention and K+ excretion (aldosterone) 3) Ca++ retention and phosphate wasting (PTH, Vitamin D) 4) pH balance (excretion or reabsorption of H+ or HCO3 A few more key concepts: 1.) Glomerular filtration pressure is a sum of all partial pressures. (Just think of Daltons law when you think of this sort of.) Here is a diagram that helps visualize it a lot better: As you can see here the hydrostatic fluid is always the natural pressure of the liquid in the vessels pushing through the membrane and the colloidal osmotic pressure is due to the proteins in each of the tissues pulling the liquids across the membranes. (note there is no colloidal osmotic pressure in lumen because there is no protein in urine.) 2.) Renal Clearance: Definition: volume of plasma from which the substance is cleared completely per unit time. Cx = Ux*V/Px • Cx = Clearance of X • Ux = urine concentration of X • V = urine flow rate • Px = plasma concentration of X If Cx < GFR, then there is net tubular reabsorption of X. If Cx > GFR, then there is net tubular secretion of X. If Cx = GFR, then there is no net reabsorption or secretion. Take for example Na+. If the clearance (CNa+) of sodium was 200L/day for example it would be higher than the GFR of 180 L/day and therefore there would be net tubular secretion of Na+, meaning that there was more sodium being excreted than there was left in the plasma. Know how inulin and creatinine are used. Some notes about the glomerular membrane: Composed of : • Fenestrated capillary endothelium (size barrier) • Fused basement membrane with heparan sulfate (negative charge barrier) • Epithelial layer consisting of podocyte foot processes The negative charge barrier is lost in nephrotic syndrome, resulting in albuminuria, hypoproteinuria, generalized edema and hyperlipidemia. -Nomally proteins cannot cross over into urine because they carry a negative charge and therefore cannot cross the negative barrier. Negative ions can cross because of their small size and can fit in the gaps in the barrier. Therefore if a person has protein in their urine it means that the negative charge barrier (the basement membrane) was destroyed.