HEALTHLINE
May 2006
NEW DRUGS/INDICATIONS
LEVEMIR (Insulin detemir [rDNA origin]) A long-acting insulin indicated for Type 1 diabetes (in
adults and children) and type 2 diabetes (in adults) when long-acting insulin is needed. Insulin
detemir is a basal (long-acting) insulin analogue with duration of action ranging from 5.7 hours at
the lowest dose to 23.3 hours at the highest dose. After SC injection, the serum concentrations
for insulin detemir indicate a slower, more prolonged absorption over 24 hours in comparison to
NPH human insulin. Maximum serum concentration is reached between 6–8 hours after
administration with a terminal half-life of 5–7 hours depending on dose. In general, patients
treated with insulin detemir achieved levels of glycemic control similar to those treated with NPH
human insulin or insulin glargine, as measured by glycosylated hemoglobin (HbA1C). In trials of
up to 6 months duration in patients with type 1 and type 2 diabetes, insulin detemir was
associated with somewhat less weight gain than NPH. Detemir should not be mixed or diluted
with other insulins. Detemir effects may be potentiated by oral antidiabetic drugs, ACE inhibitors,
disopyramide, fibrates, fluoxetine, MAOIs, propoxyphene, salicylates, somatostatin analogue, and
sulfonamide antibiotics. Detemir activity may be antagonized by corticosteroids, danazol,
diuretics, sympathomimetics, isoniazid, phenothiazines, and somatropin. Variable effects have
been associated with β-blockers, clonidine, lithium salts, alcohol. Adverse reactions may include
hypoglycemia, local or systemic allergy, lipodystrophy, and edema. DP
WARNINGS AND ADVERSE EFFECTS
Advair and Serevent Updated Label Warning
Product labels for Advair Diskus (fluticasone propionate/salmeterol xinafoate) and Serevent
Diskus (salmeterol xinafoate) have been updated to include a strict new warning that advises
physicians to limit their prescribing of the drugs to specific patient populations.
According to the FDA, long-acting beta 2-agonists (LABAs) such as these can decrease the
occurrence of asthma episodes, but make them more severe if they occur. A recent study
showed that salmeterol can increase the risk of death during a severe episode.
The new label suggests that physicians evaluate whether a patient's asthma can be adequately
controlled by using other controller drugs, such as inhaled corticosteroids (ICS), before
prescribing a LABA. The label also recommends that physicians consider whether the severity of
a patient's disease warrants initial treatment with an ICS and a LABA. SK
REGULATORY UPDATE
CMS Releases New Surveyor Guidance
On March 10, 2006, CMS published advanced copies of the State Operations Manual (SOM)
Survey Guidance on Psychosocial Outcomes, Activities, and Quality Assurance and Assessment.
All three documents discussed below have been provided as advanced copies however CMS
does not anticipate any changes. The following website can be used to access a copy of the new
guidance
to
surveyors:
http://www.cms.hhs.gov/SurveyCertificationGenInfo/PMSR/list.asp#TopOfPage>
After going to the website, the information will be listed beginning with the year 2001. Scroll all
the way to the bottom to get to the documents under 2006.
Copyright 2006
All Rights Reserved
Published by Omnicare, Inc.
distributed by PBM Plus, Inc.
Page - 1
HEALTHLINE
May 2006
Revised Activities Guidance (Tags F248 and 249)
New surveyor guidance for surveying activities requirements in long term care facilities will
become effective June 1, 2006. At that time, a final copy of the guidance will be available at
http://www.cms.hhs.gov/Transmittals/. This guidance will be incorporated into Appendix PP of
the State Operations Manual. The interpretive guidelines clarify areas such as assessment, care
planning, interventions and activity approaches for residents with behavior symptoms. Included
as a part of this document are interpretive guidelines, and an investigative protocol along with
guidelines for determination of compliance.
New Psychosocial Outcomes Severity Guide
New surveyor guidance for using the psychosocial outcome severity guide for surveying long
term care facilities will become effective June 1, 2006. At that time, a final copy of this new
guidance will be available at http://www.cms.hhs.gov/Transmittals/. This information will be
incorporated into Appendix P of the State Operations Manual. The guide clarifies when to apply
the “reasonable person concept” and included in this information are instructions and clarification
of terms along with the severity guide. The severity guide provides criteria for the determination
of the correct levels of negative psychosocial outcomes that developed, continued, or worsened
because of the facility’s non-compliance.
Revised Surveyor Guidance for Quality Assessment and Assurance (QAA) (Tags F520 and
F521) [I found this article difficult to read and certainly not at the reading level for nurses.
See if my edits will help in your opinion]
The revised surveyor guidance for surveying QAA requirements in long term care facilities will
become effective June 1, 2006. At that time, a final copy of the guidance will be available at
http://www.cms.hhs.gov/Transmittals/. This information will be incorporated into Appendix PP of
the State Operations Manual. The revised guidance provides categories of deficiencies and how
to investigate and interpret deficiencies. The guidance outlines the QAA committee composition
and frequency of meetings. As well advice is provided on how to identify quality deficiencies,
develop and implement action plans and correct identified quality deficiencies. The protocol
explains what the surveyors will need for their investigation. The deficiency categories provide
guidance for the determining the correct level of severity of outcome to residents from
deficiencies identified at Tag F520.
Compliance Statement for the Installation of Emergency Lighting and the Replacement of
Existing Roller Latches in Corridor Doors
A memorandum was sent to state survey agencies from CMS dated March 10, 2006 which
concerns several fire safety requirements related to the adoption of the 2000 edition of the Life
Safety Code. The regulation gave facilities until March 13, 2006 to comply with two changes to
the requirements. Those requirements included:
1)
Replacing batteries used in emergency lighting, where required, to provide
illumination for a minimum of 90 minutes; and
2)
Replacing roller latches commonly found in corridor doors with a positive latching
device.
Beginning with surveys completed after March 13, 2006, deficiencies concerning installation of
the 90 minute duration batteries used in emergency lighting shall be cited at Tag K46 which deals
with emergency lighting requirements. Deficiencies in the replacement of roller latches with the
Copyright 2006
All Rights Reserved
Published by Omnicare, Inc.
distributed by PBM Plus, Inc.
Page - 2
HEALTHLINE
May 2006
positive latching device will be cited at Tag K18 which includes requirements for corridor doors
and latching requirements.
To access a copy of the survey and certification letter concerning these requirements, please go
the
following
website:
http://www.cms.hhs.gov/SurveyCertificationGenInfo/downloads/SCLetter06-08.pdf
Medicare Provider Education Articles
The Medicare learning Network has renamed the provider education articles which were
previously known as “MedLearn Matters” articles, as “MLN Matters”. The MLN stands for
Medicare
Learning
Network.
The
articles
can
now
be
accessed
from
http://www.cms.hhs.gov/MLNMattersArticles. In addition, the URLs for the Medicare Learning
Network have changed and they can be reached from the cms.hhs.gov main page by clicking on
“Outreach and Education” KM
PATIENT CARE
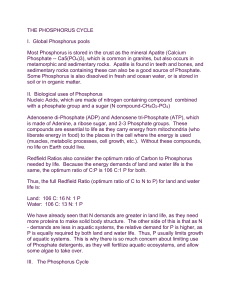
Focus on Hyperphosphatemia Associated with Chronic Kidney Disease
(CKD)
There are over 300,000 stage 5 CKD dialysis patients in the United States. These patients have
limited or no kidney function and depend on dialysis, along with dietary restrictions and
phosphate binders to minimize serum phosphorus. Hyperphosphatemia, or high phosphate blood
concentration, has been shown to significantly increase patient mortality and morbidity and can
occur in any patient with CKD. Phosphorus control is critical to the quality of care for CKD
patients.
Hyperphosphatemia and disorders of mineral metabolism are associated with progression of
CKD. This leads to an increased risk of soft tissue, vascular and organ calcification,
cardiovascular events and mortality. There are many factors affecting serum phosphorus
concentrations in CKD. These include dietary intake of phosphate, ingestion of phosphate
binders, degree of secondary hyperparathyroidism, magnitude of vitamin D deficiency and
treatment with vitamin D, dialysis (frequency, duration, and adequacy), and high intake of calcium
supplements.
In renal disease, tubular failure causes phosphate excretion to be inhibited because of the nonresponsiveness of the tubules to parathyroid hormone. Therefore, phosphate concentrations rise
while calcium concentrations fall. In addition, active vitamin D production is reduced, lowering
absorbed calcium.
The goals of therapy have become more aggressive over the past several years, because of the
high morbidity and mortality associated with altered phosphorus, calcium and parathyroid (PTH)
metabolism. It is now recommended to normalize serum calcium, phosphorus, and calciumphosphorus product in patients with CKD. The goal of therapy for serum phosphorus is to
maintain the concentration in the range of 2.5 mg/dl to 5.5 mg/dl. Patients with known or
suspected CKD should be evaluated to determine if phosphorus, calcium or PTH levels are
elevated.
Hyperphosphatemia is managed through dialysis, diet modification and utilization of phosphate
binders to inhibit absorption of dietary phosphorus. Due to the limitations of dialysis and the
Copyright 2006
All Rights Reserved
Published by Omnicare, Inc.
distributed by PBM Plus, Inc.
Page - 3
HEALTHLINE
May 2006
challenges of dietary phosphorus restriction, almost all dialysis patients rely on a phosphate
binder to reduce phosphorus absorption and prevent hyperphosphatemia. If phosphorus or intact
PTH concentrations cannot be controlled within the target range despite dietary phosphorus
restriction, phosphate binders should be prescribed. Phosphate binders bind dietary phosphorus
in the gastrointestinal tract.
Calcium-containing phosphate binders are the most common class of phosphate binders
prescribed to patients with CKD. They have the advantage in that they treat both
hyperphosphatemia and hypocalcemia. Calcium-containing phosphate binders are relatively
inexpensive. The primary disadvantage of this class of agents is that they may cause
hypercalcemia, especially when used in conjunction with Vitamin D. As many as 50% of patients
with Stage 5 CKD treated with calcium-containing phosphate binders may develop
hypercalcemia. The total dose of elemental calcium provided by the calcium-based phosphate
binders should not exceed 1,500 mg/day, and the total intake of elemental calcium (including
dietary calcium) should not exceed 2,000 mg/day.
Calcium-based phosphate binders should not be used in dialysis patients who are hypercalcemic
(corrected serum calcium of >10.2 mg/dL), or whose plasma PTH concentrations are <150 pg/mL
on 2 consecutive measurements. Noncalcium-containing phosphate binders are preferred in
dialysis patients with severe vascular and/or other soft tissue calcifications.
All are similarly effective (Table 1). Calcium-based products are often used as first line due to
their ease of administration, and limited risk of toxicity. However, non-calcium based products are
a safer alternative in patients who experience hypercalcemic symptoms or have an elevated
calcium-phosphate product (>55 mg2/dL2).
Table 1. Phosphate Binders
Compound
(Brand name)
Calcium carbonate
(Tums, Oscal, etc)
Estimate of
% Calcium absorbed
Approximately 20-30%
is absorbed
Potential
side effects
Hypercalcemia, extraskeletal
calcification, GI side effects,
constipation
Calcium Acetate (Phos- With meals: ~21%
Lo)
Between meals: ~40%
Hypercalcemia, extraskeletal
calcification, GI side effects
Sevelamer
(Renagel)
None
(noncalcium)
GI side effects
Lanthanum (Fosrenol)
None
(noncalcium)
GI side effects
Renagel (sevelamer) is a non-calcium containing phosphate binder indicated for
hyperphosphatemia in patients with ESRD. Short-term clinical studies in patients with ESRD have
established that sevelamer is as efficacious as calcium carbonate or acetate at lowering serum
phosphorus, and is well-tolerated. Furthermore, short-term control of hyperparathyroidism has
proved to be adequate, with maintenance of normal serum calcium concentrations, and in
addition, short-term favorable effects on the lipid profile have been observed, with a 20-30%
Copyright 2006
All Rights Reserved
Published by Omnicare, Inc.
distributed by PBM Plus, Inc.
Page - 4
HEALTHLINE
May 2006
decrease in low density lipoprotein (LDL) cholesterol, and a 5-15% increase in high density
lipoprotein (HDL) cholesterol concentrations, presumably related to the binding of bile acids by
the compound. This dual action is clinically significant since atherosclerosis and CVD are major
causes of morbidity and mortality in this population. Non-calcium phosphate binders, such as
sevelamer, prevent calcification of coronary arteries seen in patients with CKD that receive
calcium-based binders.
There are many complications associated with treating hyperphosphatemia. It is difficult for
patients to adhere to a low phosphate diet. Dosage titration of phosphate binders is complex
often requiring multiple tablets or capsules each day. The use of calcium-based phosphate
binders is associated with the development of hyperphosphatemia. Continued monitoring and
dosage adjustment of phosphorus binders is necessary to maintain appropriate phosphorus
concentration and to increase the likelihood of positive outcomes for the patient. Please contact
your Consultant Pharmacist for more information. KH
K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney
Disease. 2004.
_________________________________________________________________________
Contributing Authors for This Issue:
Kelly Hollenack, PharmD, CGP, FASCP
National Director Health Management
Susan Klem, BS Pharm, CGP, FASCP
Regional Clinical Director
Great Lakes and Great Plains Regions
Kelli Marsh, RHIA, RAC-C
Vice President of Support Services
Omnicare Pharmacies of Northern and Central Ohio
David Pregizer, RPh
Area Clinical Manager
NeighborCare Allentown
Editorial Board
Karen Burton, R. Ph., GCP, FASCP
Mark Coggins, Pharm. D., GCP, FASCP
Kelly Hollenack, Pharm. D. CGP
Philip King, Pharm. D., GCP, FASCP
Susan Kleim, B.S., Pharm., GCP, FASCP
Terry O’Shea, Pharm. D., GCP, FASCP
Elmer Schmidt, Pharm. D., GCP, FASCP
Barbara J. Zarowitz, Pharm. D., GCP, FASCP
Copyright 2006
All Rights Reserved
Published by Omnicare, Inc.
distributed by PBM Plus, Inc.
Page - 5