Migraine Info
advertisement

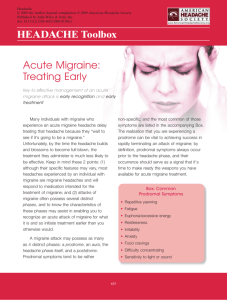
Attention to several management principles optimizes success. For "anticipated" disabling headache, episodic migraine sufferers need to intervene with migraine-specific treatment before full-blown migraine appears. Early intervention leads to reduced second doses due to reduced recurrence, reduced adverse effects, reduced absenteeism and presenteeism, and thus functional disability.[45–47] Adequate doses of medication should be used. This typically means maximal package insert doses with exceptions for very small or elderly individuals, or those exquisitely "sensitive to all medications." While practitioners maximize pain-freedom; however, they must also do no harm.[38] To fulfill this principle, headache progression must be prevented. Limiting acute treatment ideally to 2 or less days per week on average is critically important and avoids fulfilling criteria for medication overuse for any treatment as set out by ICHD-2 criteria.[48] Overall acute symptomatic treatment guiding principles are to "Treat early, ideally in less than 15 minutes, always in under 60 minutes. Treat with your best medicine for this headache type. Treat each headache acutely, but less than or equal to 2 days per week or 9 days per month. Use 2 or less doses of any given drug (ideally one and done) on average." Treatment as early as the syndrome of migraine or headache is recognized is patient dependent, but nearly always possible. In early triptan clinical trials, treatment was only initiated after migraine was fully expressed by ICHD-1 or 2 criteria; i.e., moderate or severe pain. Relief rates typically approximated 65% within 4 hours.[52] The 2-hour pain-free secondary endpoint was achieved ~30% of the time. In the Spectrum Study, a triptan relieved moderate to severe headache with the best results achieved in the headaches with the least ICHD migraine symptoms.[54,55] Further Spectrum analysis revealed greater pain freedom and lower recurrence when treating mild headache, known as early intervention.[45,46] With early intervention, 2-hour pain-free rates doubled, and in open-label extension trials nearly tripled when migraine specific triptans were compared with standard treatment protocols. One of the most common mistakes in migraine therapy is the use of an inadequate dose, whether triptan, DHE, or an antiinflammatory drug. Another mistake causing the clinical imperative to be missed is the failure to stratify to combination therapies with complementary and rational mechanisms when necessary. Prior combinations mentioned include sumatriptan-naproxen. Any triptan can be combined with an antiinflammatory drug with significant benefit commonly derived