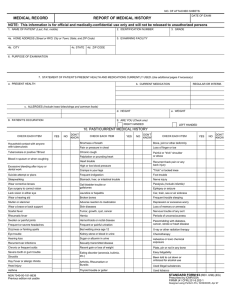
REPORT OF MEDICAL HISTORY
advertisement

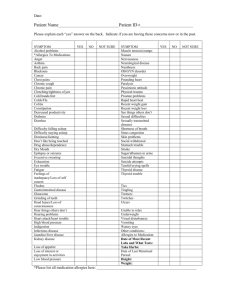
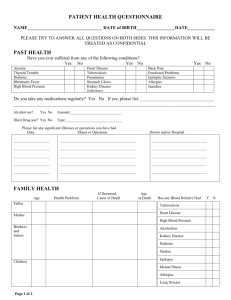
PART 2 - MEDICAL HISTORY REPORT ( To be filled in by examining doctor ) NAME OF APPLICANT: ____________________________ NRIC / PASSPORT NO: _____________________________ HOME TELEPHONE NO: __________________________________ ADDRESS: __________________________________ This course is strenuous in nature and may require the trainee to don personal protective equipment, breathing apparatus etc in confined space during the training process. The purpose of these questions is to ensure that the trainee does not have any medical condition which would place him/her at an increased risk during training. HAVE YOU EVER HAD OR DO YOU NOW HAVE: ……………. Please mark each item below “Yes” or “No”. All “Yes” items must be fully explained in Para 10 Yes 1a. Asthma or any breathing problems related to exercise, weather pollens, etc. b. Shortness of breath c. Bronchitis d. Wheezing or problems with wheezing e. Sinusitis 2a. b. c. d. Painful shoulder, elbow or wrist Recurrent back pain or any back problem Foot trouble (e.g. pain, corns, bunions, etc) Knee trouble (e.g. locking, giving out, pain or ligament injury, etc) e. Bone, joint, or other deformity f. Broken bone(s)(cracked or fractured) 3a. b. c. d. Stomach, liver, intestinal trouble, or ulcer Gall bladder trouble or gallstones Jaundice or hepatitis (liver disease) Rectal disease, hemorrhoids or blood from the rectum Frequent or painful urination High or low blood sugar Kidney stone or blood in urine Sugar or protein in urine e. f. g. h. 4a. Pain or pressure in the chest b. Palpitation, pounding heart or abnormal heartbeat c. Heart trouble or murmur d. High or low blood pressure 5a. b. c. d. Dizziness or fainting spells Frequent or severe headache A head injury, memory loss or amnesia Seizures, convulsions, epilepsy or fits No Yes 6a. Nervous trouble of any sort (anxiety or panic attack) b. Loss of memory or amnesia, or neurological symptoms c. Depression or excessive worry d. Been evaluated or treated for a mental condition 7. … Have you ever been a patient in any type of hospital? No If yes, please specify when, where and why: _________________________________________ _________________________________________ 8. FEMALES ONLY. Have you ever had or do you now have: a. Treatment for a gynecological (female) disorder b. A change of menstrual pattern Have you ever had any illness or injury other than those already noted? 9. If yes, specify when, where and give details: _______________________________________ _______________________________________ 10. If any of the above answers is “Yes”, please provide explanation below . ___________________________________________________________________________________________________ ___________________________________________________________________________________________________ EXAMINED BY: NAME OF DOCTOR: _____________________________________ SIGNATURE & STAMP::_________________________ NAME OF HOSPITAL / CLINIC: ____________________________ ADDRESS: ___________________________________ DATE: ______________________________________________ TELEPHONE: ___________________________________