KURBAN CHIROPRACTIC HEALTHCARE CLINIC
advertisement

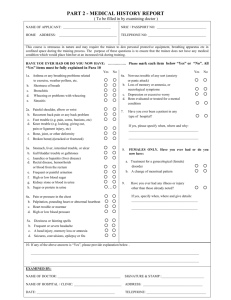
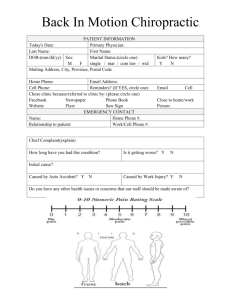
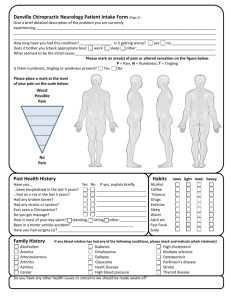
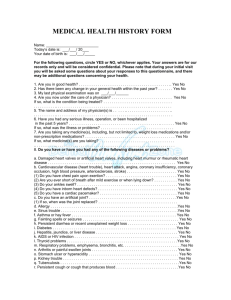
CONSENT TO EXAMINATION AND DETERMINATION OF A CHIROPRACTIC CASE The taking of a history and physical examination are not considered treatment, but are part of the process to determine if your case will benefit from chiropractic care. If Dr. Hughlett or any Associate Doctor does not believe that your condition will respond to chiropractic care, she/he will not accept you as a patient but will, if appropriate, refer you to another health care provider. If your case requires immediate attention, emergency first aid and/or therapeutic adjunctive procedures will be performed. I hereby request/authorize Dr. Michael Hughlett, and/or any Associate Doctor to perform diagnostic examination tests and x-rays, and if necessary, to perform emergency first aid and/or therapeutic procedures to myself. /my minor child: Signature: Date: PATIENT INFORMATION PATIENT NAME: TODAY’S DATE: Age: Sex: Female / Male Past Chiropractic Care No / Yes: When? Previous Chiropractor’s Name: Results? Are your present problems due to an injury? No/ Yes: On the Job Auto Accident Personal Injury Other: Has the accident been reported? No / Yes: to Employer to Auto Carrier Other: Are you now or have you ever been disabled? (service or work)? No / Yes: When? Why? Have you retained an attorney? No / Yes: Name & Address: HISTORY OF PRESENT ILLNESS Chief Complaint: When did it first start: How long does it last? What make it worse? What make it feel better? Does it hurt more in the morning, afternoon or evening? Explain: Has this ever happened before? Explain: Are you taking any medication for this pain? Are there other associated problems? Please circle the intensity for the Please mark area & type of discomfort on the drawing using the codes below: pain you described above: N=Numbness 1. Chief Complaint: ST=Stiffness 1 2 3 4 5 6 7 8 9 10 S=Soreness 2. Associated Problems: A=Ache 1 2 3 4 5 6 7 8 9 10 T=Tingling 3. Associated problems: P=Pain 1 2 3 4 5 6 7 8 9 10 OPERATIONS AND PROCEDURES I have never had any operations/surgeries. Prior Surgery and Dates: Vaccinations: Tubes in Ears: Sinus: Stomach: Appendectomy: Hernia: Thyroid: Back Operation: Rectal Surgery: Tonsillectomy: _______ Female Organs: Gall Bladder: HAVE YOU HAD, OR DO YOU HAVE ANY OF THE FOLLOWING CONDITIONS? Mental Disorder Whooping Cough Migraine Headaches Heart Disease Cancernn Anemianm Pleurisy n Polionnn Asthmannn Influenzam Goiternn DiabetesnnnMumpsmn Arthritism HIV Positive Epilepsy Pneumonia Measles Eczema Chicken Pox Appendicitis Alcoholism Tuberculosis Lumbago Venereal Disease Multiple Sclerosis Rheumatic Fever Herpes SOCIAL HISTORY Marital Status: Single Married Widowed Divorced Alcohol Use: No / Yes: How Much? Tobacco Use: No / Yes: How Much? Activity: Sitting Standing Light Labor Heavy Labor Occupation: Caffeine Use: No / Yes: How Much? Exercise: None Light Activity Moderate Activity Work Active Very Active Elite Athlete REVIEW OF SYSTEMS Please check the correct box for each item below. -Previously -Presently General Symptoms -Allergy (what) Respiratory -Chest Pain -Chronic Cough -Difficulty Breathing -Spitting Blood -Spitting Phlegm -Bronchitis -Chills -Convulsions -Dizziness -Fainting -Fatigue -Fever -Headache -Loss of Sleep -Loss of Weight -Nervousness -Neuralgia -Sweats -Wheezing -Depression Gastro-Intestinal - Belching/ Gas/Bloating -Abdominal Pain -Constipation -Diarrhea -Excessive Eating -Gall Bladder Trouble -Hemorrhoids (piles) -Jaundice -Liver Trouble -Nausea -Stomach Pain -Poor Appetite -Poor Digestion -Vomiting -Vomiting Blood -Excessive Thirst -Indigestion -Rectal Bleeding Muscles/Joints/Bones -Backache -Foot Trouble -Hernia -Pain Between Shoulders -Painful Tail Bone -Stiff Neck -Spinal Curvature -Swollen Joints -Tremors/Twitching -Arm Trouble Eye/Ear/Nose/Throat -Asthma -Crossed Eyes -Deafness -Earache -Ear Discharge -Ear Noises -Enlarged Thyroid -Frequent Colds -Hay Fever -Hoarseness -Nasal Obstruction -Nosebleeds -Pain in Eyes -Poor Vision -Sinusitis -Sore Throat -Tonsillitis -Persistent Cough -Difficulty Swallowing -Bleeding Gums Cardio-Vascular -High Blood Pressure -Low Blood Pressure -Pain Over Heart -Poor Circulation - Heart Trouble -Rapid Heart -Slow Heart -Strokes -Swelling Ankles Skin or Allergies -Boils -Bruising Easily -Dryness -Eczema -Hives or Allergy -Itching -Sensitive Skin -Skin Eruptions Genito-Urinary -Bed Wetting -Blood in Urine -Frequent Urination -Lack of Bladder Control -Kidney Infection -Painful Urination -Prostate Trouble For Women Only -Cramps or Backaches -Excessive Flow -Hot Flashes -Irregular Cycle -Miscarriage -Painful Periods -Vaginal Discharge -Lump in Breast Pregnant at this time? Yes/No Last Menstrual Period? Last PAP? By whom? Have you had a mammogram? Yes/No # of Pregnancies # of Deliveries PAST HISTORY List any accidents or falls and dates: Car Recreation Sports School Other List any broken bones (fractures) or dislocations: Have you ever been on crutches? No / Yes Why? Have you ever had spinal taps or spinal injections? No / Yes Were you ever knocked unconscious? No / Yes Have you ever had a lapse of memory? No / Yes Have you ever had x-rays taken? No / Yes: When? By Whom? For what ailments were these x-rays taken? Do you suffer from any condition other than that which you are now consulting us? Are you presently taking any medications – prescription or over-the-counter? No / Yes: Please list: FAMILY HISTORY Mother Father Brother, # Sister, # of of Diabetes Heart Attack High Blood Pressure NOTES Kidney Cancer Other