Hendershot, E. (2005). Outpatient
advertisement
. Outpatient")
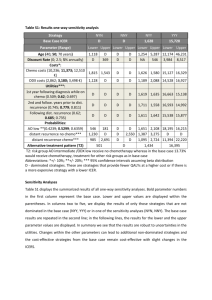
Declare the Aim The GRRCC Systemic Wait Time Reduction Project attempts to reduce the wait times for patients receiving chemotherapy. Prior to the project, a rolling 3 month median wait time of 5.5 weeks from referral to treatment was reported for Grand River Regional Cancer Centre (GRRCC) systemic therapy patients. The project attempts to achieve a wait time target for 2007 / 2008 in which 70% of our new patients start systemic therapy treatment within 4 weeks of referral. Wait times are an important indicator of how quickly our patients are getting access to cancer care. Once a cancer diagnosis has been made, the wait for the treatment phase begins. One part of that treatment is systemic therapy. Systemic therapy plays a vital role in either prolonging life or by increasing a patient’s quality of life through the reduction of symptoms. Removing barriers to treatment is essential so patients have timely access to the appropriate course of treatment. These wait time measures also indicate GRRCC’s ability to meet the needs of all cancer patients within its catchment area, providing treatment close to home. Despite the increasing demand and chemotherapies being prescribed, wait times for chemotherapy remain stagnant across the province. Timely access to high-quality cancer treatment leads to improved treatment outcomes, prognosis, quality of life, and satisfaction with care. Waiting for treatment can be emotionally difficult and stressful for patients and their caregivers. “In the few studies that have explored the setting of cancer care, long wait times are frequently linked to dissatisfaction.” (Hendershot, 2005). Potential areas have been identified for improvements related to wait times. Possible solutions / opportunities included investment in information technology and information management, efficiency improvement, and better utilization of services. By facilitating the process of each individual step from booking to the actual treatment, wait times can be reduced. It is the goal of the GRRCC to create a smoother, timelier scheduling process by increasing efficiencies and this is planned to be achieved by introducing five sub-aims (for further detail see change section below) i. ii. iii. iv. v. Referral to consult wait time within 2 weeks for 80% of our patients Reduce waste in the process of orders Create designated spaces for urgent/emergent patients (to provide sufficient new patient consult capacity by enabling Medical Oncologist / Hematologist to handle new patient and emergency consults as their top priority) Increase flexibility in handling add-on and non-chemo support care treatments (to more fully utilize the chair capacity of the systemic therapy suite) Ensure patients are on their first treatment within 3 days of the decision to treat Simplified Process Flow – Bottlenecks (red boxes) / Implemented Solutions (Yellow Circles) 1) Ref er new patient to the Centre f rom Physicians or DAU 3) Triage the new patient by Rad Onc or Med Onc and returns package to NPR to schedule consult (if required) 2) Assemble a Triage package by New Patient Ref errals and sends to appropriate Oncologist 4) Schedule a consult and advise Ref erring Physician or MedOnc who advises the patient. 6) Conduct scheduled and unscheduled consults conduct nursing assessments and make a DTT (If possible) or schedule additional tests or arranges supportive care by the Med Onc. S1 5) Scheduled new patient arrives at Main Reception S2 7) Schedule additional testing & f ollow-up appointments if required & advises patient by Clerical Staf f 8.1) Conduct f ollow-up clinic visits if req’d by Med Onc 9) Patient makes decision about treatment and advises Physician or nurse to schedule chemo appointments (RTT) 10) Order meds in OPIS & prepares a Green sheet dated as per prep date, orders prescription, or prepares a paper order by Med Onc 8) Conduct testing S2 11.1) Book Procedures in the Chemo Suite & advise patients 12) Install central line access or conduct other procedures (if required) 11.2) Schedule Return Patients & Lab tests and advise patients 13) Check chemo orders by Chemo Nurse 11.3) Establish start date f or treatment Book Chemo, Blood App’t & Chemo teach & advise patients 14) Verif y orders and change start date as determined by booking clerk by Pharma 11.4) Establish start date f or Chemo & Radiation when co-modality treatment is required and advise patients 15)Conduct patient blood draws at blood lab or in Chemo Suite and blood work by Blood Lab 16) Conduct chemo teach with patient S2 17) Scheduled, Unscheduled or Emergency Patient arrives Front Desk, Blood Lab, Clinic or Chemo. S3 18) Conduct pre chemo teach with patient by Pharma 19.2) Conduct assessments, consult with MD (if req’d) & deliver other Supportive Care treatments as req’d by Nurse 19.1) Seat patient, assesses patient, checks blood work, consults with Dr or Pharma (if req’d), places pre printed meds orders in Pharma door and preps f or chemo delivery by Nurse 20) Print orders f or the day, check blood results, consult with Dr. (if req’d) and prepare meds 21) Monitor Pharma meds preparation, pick up when ready, conduct cross ref . with OPIS, check drug, dose & calc. by Nurse 22) Administer the meds and monitor patient by Nurse 24) Pick-up take home meds at Pharma by Patient 23) Discharge patient af ter conf irming next app’t, and take home meds (if req’d) Measure Improvement According to Cancer Care Ontario (CCO), “the waiting period from the time a hospital’s regional cancer centre receives a referral for a patient to receive systemic treatment to the time the patient receives his or her first treatment” is referred to as “referral to treatment”. “Referral to treatment” wait times are reported by median, in days (i.e. the point at which half the patients have had their treatment and the other half are still waiting) and all time intervals longer than 20 weeks are excluded. The Cancer Care Ontario’s Expert Wait Time Committee announced a wait time target for systemic treatment and it is consistent with the Canadian Association of Radiation Oncology standard. Our benchmark is CCO’s target since it is crucial for patients to receive treatment within the recommended time frame to ensure best outcomes. ACCESS CSQI 2007 CSQI 2008 Ontario Min Max Target *Systemic treatment waits: Median wait (in days), referral to start of systemic therapy treatment 39.2 32.9** 32.9 73 37.8 28 Source: CCO website. The chart below shows the indicators that are measured monthly to assess our progress toward our aim. Indicator Rationale Data Source Indicates efficient and Monthly appropriate patient handling reports Consistent with CCO from OPIS metrics and OHS Indicates efficient and Monthly appropriate patient handling reports Consistent with CCO from OPIS metrics and OHS Indicates availability of NP Monthly consult slots report from OPIS Baseline Current (May 07) (Aug 08) 50% 63% (May 08) Target 5.2 wks 3.8 weeks (Oct 07) (June 08) 4 weeks 58% 65% (June 08) 80% 76.3 Unable to get 95% current # due to staff shortages. Manual calculation available Sept 19/08. 47% 70% (Aug 08) % of patients who start their chemo treatment within 4 weeks of Referral Median wait in weeks from referral to first treatment • % of patients who have their consult appointment within 2 weeks of Referral % of orders processed within 24 hours of receipt • • Indicates efficient booking of treatment Quarterly manually % of new patients starting treatment within 3 working days of Ready to Treat % of emergency patients seen within a week • Indicates efficient patient flow into the chemo suite and supportive care area Monthly 24% report from OPIS • Indicates timely handling of Monthly NA emergency patient consults report from PHS • • • Improved from baseline. Achieved Target 100% breast 0% GI 100% lung (May-Aug 08) 70% 90% Share the Results The project was initiated in April 2007. Over the course of one year, systemic therapy median wait times have shown to trend down. Our data shows that the wait time started to decline and stabilize starting November 2007, and we reached our goal of within 4 weeks in Dec/07, Feb/08, Mar/08, Apr/08, May/08, and June/08. Approximately, 50 patients start to receive treatments each month. Systemic Therapy Wait Times 6 In Weeks 5 4 3 2 1 0 Apr- May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- May- Jun07 07 07 07 07 07 07 07 07 08 08 08 08 08 08 Period Wait Time Benchmark Additionally, these changes have resulted in an increased number of patient’s starting systemic therapy treatment. In the period between April - June 2007 GRRCC accepted 471 new patients. During the same time period (April - June) in 2008, GRRCC was able to accept 546 new patients, well surpassing the budgeted volumes. Similarly, the number of new case visits also increased: Systemic Therapy # of new case visits (C1S) Budgeted Volume 2007-2008 1,858 Q4 YTD Actual Volumes 2006-07 1,798 2007-08 1,980 % Variance 6.6% While improving the wait times for systemic therapy, GRRCC has also managed to increase staff and patient satisfaction with the new process. The following is a list of quotes: New Patient Referral Staff: “The surgeon’s offices are generally surprised by the short wait to see an oncologist and are delighted for their patients” Clerical staff in the clinics: “It is a lot easier to book patients into the chemotherapy suite compared to last year. There seems to be more time available” Clerical staff in the chemotherapy suite: “The patients are pleased with the changes in the supportive treatment area, they say they don’t have to wait as long in the waiting room when coming to get lab work drawn from their PICC lines”. Patient response for first chemotherapy visit “Oh wow – I didn’t expect my first treatment to be booked that early” (the appointment was booked the same week that the pt saw the oncologist) Hematologist “Since the changes have been made it has been easier to treat patients with urgent needs – either chemotherapy or supportive treatment. These patients are being accommodated much faster.” “The new way that the bone marrows are organized is working out really well for the physicians and the patients. Thanks for that.” Identify the Changes Solution 1 (S1) – Proactively monitor and adjust NP slots to meet DS patient volumes – Have some follow-ups and assesses seen by someone other then an Oncologist for all sites so the Oncologists can see new patients. Solution 2 (S2) – One secretary processes all of the orders for a particular patient group using a complexity scale – Book patients to the space – Create a complexity scale for all protocols and include acuity (A,B,C,D,E) chosen by either chemo nurse or physician Solution 4 (S4) – Establish a separate supportive care unit within the Chemo Suite Solution 3 (S3) – Have designated slots for each Oncologist to handle emergency patients based on site group needs 3 weeks Referral 24 hrs Consult Schedule Treatment 4 days 1st Treatment We implemented seven high impact changes organized into 4 solutions into the systemic therapy process: First, we planned to schedule consults within two weeks of referral 80% of the time by having some follow-ups and assesses seen by someone other then an Oncologist for all sites so the Oncologists can see new patients. This wait time is associated with the most patient anxiety. Prior to the project implementation, only 58% of patients were seen within 2 weeks. Second, we strived to reduce the number of people who process orders for a single patient by having one secretary process all of the bookings and orders for a particular patient group using a complexity scale. Large amount of errors is likely to occur in the booking process when many people have to handle a single booking. Also the handoff of a patient file to multiple secretaries to complete complex bookings often led to extensive delays. Having 1 person handle all bookings for the patient was intended to streamline the booking process. To keep the process safe for clerical staff to process all orders, a complexity scale for all protocols was developed and includes acuity (A,B,C,D,E) chosen by either chemo nurse or physician. Ultimately, these changes were put in place so we can get patients on their first treatment within 3 days of the decision to treat (DTT). This complexity scale is an important factor in scheduling realistic time to administer chemo therapy or other supportive care procedures. In the past, our lack of ability to match patient needs with the resources led to underutilization of the chemo suite. As patient volumes increase this situation was expected to result in increased wait times for chemo treatment delivery. Third, we have designated slots for each Oncologist to handle emergency patients based on site group needs so we can handle urgent, emergency and add-on consults in a timely way. In the past urgent or emergency patients where scheduled into already fully booked clinics. This situation created extensive delays in a clinic schedule with increased with the resulting increase in patient dissatisfaction. Lastly, we hoped to increase our flexibility in handling add-on and non chemo supportive care treatments in the suite by having a separate transfusion unit and possibly a bone marrow unit. If we could manage these patients differently, it would increase the capacity for chemotherapy. Sustainability The success in radiation wait time reduction at GRRCC spread the attempts to improve systemic therapy. Now that GRRCC has seen success in reducing two aspects of cancer treatment the organization has developed a culture that knows that improvement is possible. A critical success factor of this project was our ability to engage all key functions in the decision making process. It is impossible to implement effective change unless active support is developed leading up to implementation of the solutions. Many of the solutions were straight forward and had been discussed before. The engagement process built ownership and commitment to the critical stage of implementation. It is critical for GRRCC to build on this success and use the tools developed in the initial project – the Simplified Process Flow Chart, the Report Card and the multifunctional Steering Committee structure identify new opportunities and respond by implementing ongoing change that counts. Another key to the success of this project, was the fact that the Solution Sub Teams created and the Steering Committee a selected solutions which could be implemented within a 30 to 60 day time frame. This sense of urgency was instrumental in developing and maintaining implementation momentum. Longer term strategic solutions are important; however it is important that staff see tangible improvement quickly. This builds confidence and generates additional support for a sustainable change making process. Finally, an important learning that we will want to apply in the future is that it is very risky to assume that we know where the important improvement challenges are without collecting confirming data. The Steering Committee identified 5 important process improvement opportunities, however they altered 4 of the 5 after they had a chance to review targeted performance data on the process. The implications are clear. Had we not invested time at the front end we would have been trying to solve the wrong problem. To continue moving forward we need to provide the oncologists with sufficient new patient and emergent/urgent treatment slots by offloading follow-up and assesses to general practitioners, nurse practitioners, and clinical nurse specialists. One of the key changes required to support sustainability of this project is a constant monitoring of patient volumes and projected future demand. It is absolutely essential for GRRCC to be in front of the demand curve to ensure we have enough staff and treatment spaces to meet the increasing demands. The process is ever evolving. The business plan was written for over 5 years to ensure it was sustainable. Now that the project is up and working well, multi-disciplinary team needs to adopt the new process (changes) into their everyday practice. The project plan will continue to grow and improve to accommodate future changes. Reference Hendershot, E. (2005). Outpatient chemotherapy administration: Decreasing wait times for patients and families. Journal of Pediatric Oncology Nursing. Vol. 22, No. 1.