ASTHMA INFORMATION FORM
advertisement

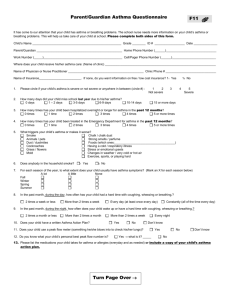
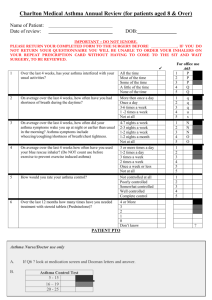
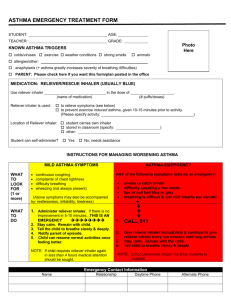
ASTHMA INFORMATION FORM Student’s Name: _______________________________ Grade: ____________ Asthma Triggers: (Check all that apply) __ Exercise __ Pollen __ Strong odors __ Change in temperature __ Mold __ Respiratory Infections __ Animals __ Food: _____________ __ Carpet __ Other: _____________ Describe the symptoms your child experiences (e.g. wheezing, coughing, tightness, other):_____________________________________________________________ What usually helps if an attack occurs? ___________________________________ Medications child takes at home for asthma: Medication Name: Dose: How Often: _____________________ ___________ _______________ _____________________ ___________ _______________ Side Effects of Medications? ____________________________________ Does your child use a peak flow meter? ________ Current Best Peak Flow: _________ Number of times child has visited an ER for an acute asthma attack in the last year _____ Additional information/instructions: __________________________________________ Signature of parent/guardian: _________________________ Date: ________________ *All medications brought to school must be accompanied by a written doctor’s order, with a signed parental permission note. The medication must be in its original container, clearly labeled, from your pharmacist. Forms are available from the school nurse, or can be located on the school website under school life/health forms. PLEASE COMPLETE THE OTHER SIDE OF THIS FORM EMERGENCY CARE PLAN: ASTHMA Student: ________________ Grade: ____ School Year: ________ DOB: _________ Mother/Guardian Phone: (H) ________________ Father/Guardian Phone: (H) ________________ Other Emergency Contact: ___________________ Student’s Doctor: _________________________ Doctor student sees for asthma: __________________ Signs of an asthma attack include: -Difficulty catching breath/ chest tightness or pain -Itchy chin or neck/ “neck feels funny” -Difficulty breathing/ rapid breathing -chest/neck pulled in with breathing -lips or nails turn blue or gray (C) __________________ (C) __________________ Phone: _______________ Phone: _______________ Phone: _______________ -coughing/wheezing -child appears restless/anxious -child is hunched over -stops activity and sits still Action: 1. Stop activity and assist to an upright sitting position. 2. Call the school nurse or school administration if the nurse is not available 3. The nurse can give an inhaler/nebulizer, or a self-directed student can use his/her own inhaler. 4. Student may return to class if symptoms are relieved. IF SYMPTOMS WORSEN: 5. Do not leave student alone 6. Call 911 7. Call parent/guardian Emergency asthma medications: Medication ordered: _________________________ Dose: _______________ Special Instructions: __________________________________________________ __ Check here if a spacer is used with a metered dose inhaler __ Check here if student has demonstrated proper use of the inhaler to the school nurse and is allowed to self-carry and administer. Written by: ______________________________________ Date: _______________ Signature of parent/guardian: _______________________Date:_________________ *Parent signature denotes permission to share the above information with staff on a need to know basis, as well as gives permission to speak to the child’s physician as needed. FASNY2015