DI-Chest-CHF
advertisement

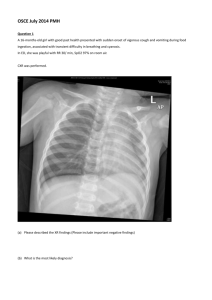
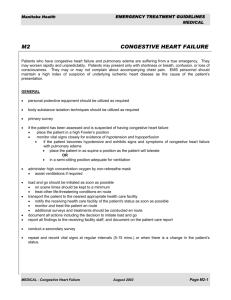
RADIOLOGY CASE REPORT Patient ID: TOH 2925762-3 Date of Study: Nov. 26, 2007 Type of Study: Portable Chest Xray (Erect AP view) 1. Clinical Indication: 91 year old female presented with chest pain. 2. Picture: Kerley B lines 2. Describe the radiological findings: - Kerley B lines - Pulmonary vascular redistribution - Increased interstitial markings at the lung bases - Tiny left pleural effusion. - The cardiomediastinal silhouette is grossly within normal limits - Atherosclerosis of the aortic arch. - Thickening of the right horizontal fissure 3. Provide possible diagnosis(es): Kerley B lines are 1-3 cm long and less then 1 mm thick, these horizontal lines perpendicularly meet the pleural space. The lines are seen usually as a ladder up the side of the lungs beginning at the costophrenic angle. These linear opacities represent fluid distended interlobular lymphatics and their surrounding connective tissues. The sum of the radiological findings suggest that the most probable diagnosis here is Congestive Heart Failure. Differential diagnosis for Kerly B lines: Raised pulmonary venous pressure due to: Congestive Heart Failure (usually left sided heart failure) Mistral Stenosis Lymphatic Obstruction due to: Pneumoconiosis: fibrosis and scarring of the lungs due to repeated inhalation of occupationally associated dust, such as silica, asbestos, and coal dust. Lymphangitis carcinomatosa Parasitic infection Sarcoidosis 4. What would you recommend next for this patient? Treatment for Congestive Heart Failure: ACE inhibitor, Beta blocker, Spironolactone, diuretics, diet and exercise. 5. Is the use of this test/procedure appropriate? Yes a chest xray is an appropriate initial test to do to view both the lungs and the heart for obvious abnormalities or evidence of heart failure. 6. Is(are) there any alternate test(s)? Blood work looking for evidence of decreased perfusion to vital organs or a myocardial infarction: ↑BUN, ↑Cr, ↓serum Na, abnormal LFTs, CK, TnT Echocardiogram: to assess ejection fraction and chamber size looking for systolic dysfunction, as well as hypertrophy, abnormal valves, and pericardial abnormalities PA catheterization: looking for signs of low-output failure (↑PCWP, ↓CO and ↑SVR) ECG: findings indicative of coronary artery disease, left ventricular hypertrophy, left atrial enlargement, or heart blocks 7. How would you explain to the patient about the possible risks and benefits of this test? A chest xray is performed using low dose radiation and therefore adds to the risk of cancer but the risk is very small that the benefits outweigh the risk. The benefits being that it provides an image of the lungs and heart simultaneously allowing for the physician to assess both organs and look for abnormalities that may be causing the patients symptoms and also aid to recommend therapy. 8. What is the cost of this test? The approximate cost of a chest xray varies anywhere from 40 – 110 canadian dollars. References: Chapman S, Nakielny R. Aids to Radiological Differential Diagnosis. Fourth edition. Toronto 2003. Sabatine M.S. Pocket Medicine. third edition. New York: Lippincott Williams & Wilkins; 2008. p1-14.