Thoracic Trauma
advertisement

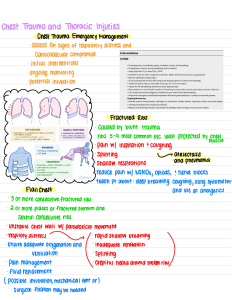
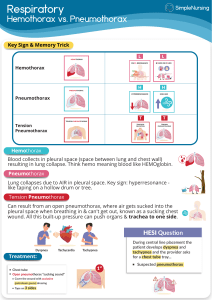
Trauma to the chest are some of the most life-threatening conditions that present to the ED. Acceleration and Deceleration forces are a common cause of intrathoracic injury. Most common type of injury is blunt trauma resulting from MVC. Isolated injury is uncommon-frequently associated with head, abdomen, or extremity injury as well. Ineffective ventilate can occur due to structural injury, pain, inability to maintain negative intrapleural pressure. Inury to thoracic vessels can cause hemorrhage and shock. Air and blood can accumulate in the thoracic cavity increasing intrapleural pressure which might cause the heart and vessels to shift or occlude. A fracture of two or more sites on two or more adjacent ribs, or when rib fractures produce a free- floating sternum. Movement of the chest wall is paradoxical during inspiration and expiration. Injury to the chest results in accumulation of air in the pleural space with the subsequent loss of the negative intarpleural pressure. This can result in partial or complete collapse of the lung. An open pneumothorax results from a wound through the chest wall that allow air to enter the pleural space both from the wound and the trachea. Tension Pneumothorax allows air to enter the pleural space on inspiration, but air cannot escape on expiration. Rising pressure causes collapse of the lung and a mediastinal shift that compresses the heart, vessels, trachea, and unaffected lung. Accumulation of blood in the pleural space. Hemorrhage can occur causing mediastinal shift, hypotension. Indications for surgery: › Volume of blood drained › Continued blood loss > 200 ml/he in first two hours. › Hemodynamic stability Simple Pneumothorax-Chest tube insertion (Thoracostomy) If pneumo < 25% may be deferred unless needs air transport. Insertion site 4th or 5th intercostal space anterior to midaxillary line. Open Pneumothorax-Cover wound with a sterile non porous dressing, taped securely on three sides. Hemothorax-Chest Tube Insertion, be prepared for large quantity of blood Tension Pneumothorax-Immediate Needle decompression (Thoracentesis) 14 gauge needle in 2nd intercostal space midclavicular on the affected side. Assessment of chest tube: FOCA › › › › F Fluctuation in the water seal chamber O Output C Color A Air leak ● Trouble shooting for problems with tubes: DOPE D – Dislodgement O – Obstruction P – Pneumothorax E - Equipment Potentially life threatening-Either from penetrating or blunt trauma Left side is more common as right is protected from the liver. Herniation of abdominal contents can occur into the thorax. Herniation results in respiratory compromise. Collection of blood in the pericardial sac. Accumulation of blood exerts pressure on heart with inhibits the ventricles ability to fill. Result from blunt or penetrating trauma There is an 85% mortality prior to arrival at a hospital. From those admitted and who received surgical intervention, an additional 10% to 30% will die. MOI is a combination of shearing and deceleration. “Cardiac Contusion” Suspect if associated MOI or has a poor cardiovascular response. Injuries may range from petechiae to fullthickness contusions to rupture of the heart