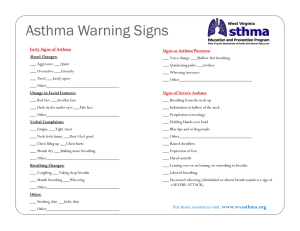
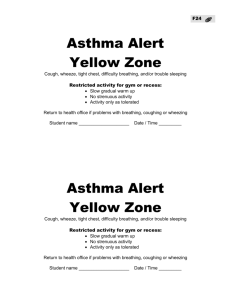
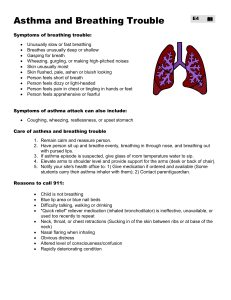
Asthma Action Plan
advertisement

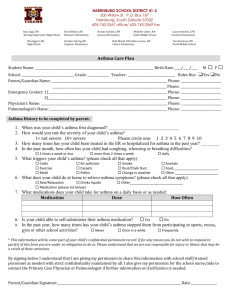
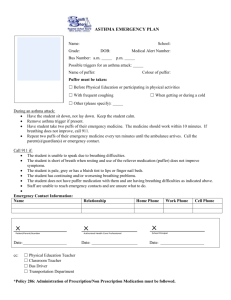
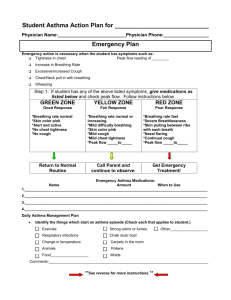
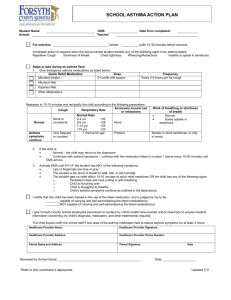
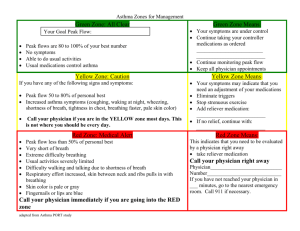
Tuloso-Midway ISD Health Services SCHOOL ASTHMA EMERGECNY ACTION PLAN Student’s Name ______________________________________ Grade _____________ Date of birth ______________________________ ID# _________________________ Emergency Contact ________________________________________________ Phone: (H) ________________ (W) ___________________ (C) _________________ Doctor’s Name _________________________________ Phone __________________ USUAL ASTHMA ACTION PLAN Usual signs of student’s asthma: Wheezing Tightness in chest Coughing Difficulty breathing Difficulty speaking Yes Yes Yes Yes Yes What triggers student’s asthma: No No No No No Exercise Yes No Colds/virus Yes No Allergies Yes No other triggers ______________ Worsening sings of student’s asthma: Wheezing Tightness in chest Coughing Difficulty breathing Difficulty speaking Medication Yes Yes Yes Yes Yes No No No No No Asthma Medications Dosage School Home I give permission to my child’s school to administer emergency medications as necessary, in accordance with the attached physician’s instructions. Parent Signature ________________________________ Date ______________ TO BE COMPLETED BY PHYSICIAN *********************Asthma Emergency Action Plan******************* Emergency action is necessary when this student has symptoms such as: 1. _____________________________________________________________ 2. _____________________________________________________________ 3. _____________________________________________________________ 4. _____________________________________________________________ Steps to take during an asthma episode: 1. Give emergency medication: A. Bronchodilator (quick relief medication) Medication: ___________________________ Dosage: ______________________________ Can be repeated for severe breathing difficulty _______ times ______minutes apart. Call 911 or EMS if minimal or no improvement 2. Seek emergency medical care if this student experiences any of the following: If no improvement 15-20 minutes after initial treatment with medication and family cannot be reached. Student exhibits: o Chest and neck pulled in with breathing o Hunched over while breathing o Struggling to breathe o Trouble walking or talking o Lips or fingernails turn gray or blue Special Instructions: _______________________________________________________ _____________________________________________________________________________ ________________________________________________________________________ Physician’s Signature:____________________________ Date ___________