health history - George Junior Republic
advertisement

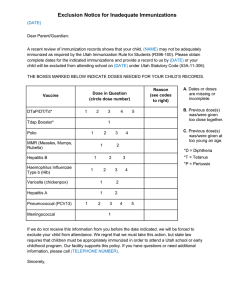
FORM 13 Page 1 HEALTH HISTORY Youth Last Name Youth First Name / / Date of Birth County / Placing Agency Having accurate medical background information at the time of admission assists our medical staff in planning and providing the best possible care for each youth. Please complete this form. Include the names and telephone numbers for all medical/dental providers who continue to provide specialized care for the above-referenced youth. Family Health History: Please check below if the grandparents, aunts/uncles, parents, or siblings have the following health conditions: diabetes heart disease stroke asthma hepatitis sickle cell disease / trait HIV infection cancer heart attack blood clots seizures / epilepsy high blood pressure depression death by suicide tuberculosis thyroid disease alcohol / drug addiction Other: Youth Health History: Please check all that apply. asthma seizures / epilepsy chicken pox hearing problems suicide attempt(s) diabetes heart condition vision problems speech problems injuries (explain below) enuresis (bed wetting) loss of bowel or bladder control headaches, migraines depression surgery (explain below) No known allergies Allergies to the following medications: Allergies to the following foods: Other allergies: CURRENT MEDICATIONS Name of medication Daily dosage/times given Reason for taking FORM 13 Page 2 YOUTH LAST NAME, FIRST NAME INSURANCE INFORMATION Primary Insurance Name Policy / Agreement # Group # Name of Policy Holder: Secondary Insurance Name: Policy / Agreement # Group # Name of Policy Holder Coverage Employer: Coverage Employer: Is youth currently receiving state medical assistance? Yes No Under the Pennsylvania Department of Human Services Guidelines, the following immunizations are required by all children, grades K-12: 4 doses of diphtheria (1 dose on or after the 4th birthday) 2 doses of varicella (chickenpox) or evidence of immunity 3 doses of polio 3 doses of hepatitis B 2 doses of measles 1 dose of rubella (german measles) 7th Grade ADDITIONAL requirements for every child include: 1 dose of meningococcal conjugate vaccine (MCV) 1 dose of tetanus, diphtheria, acellular pertussis (Tdap) IF five (5) years have passed since the last tetanus immunization was given. Please attach a copy of the youth’s immunizations with this Health History form. If you do not have this information, list the name, city, and state of the public school the youth most recently attended. Name of School City State Zip Please note below the names, phone numbers, and treatment provided for any medical, dental, psychiatric, or other health provider who recently cared for this youth. Name Phone Number / / / / / Treatment Provided / / / / / 233 George Junior Road P.O. Box 1058 Grove City, Pennsylvania 16127 724-458-9330 Ext. 2100 Fax: 724-458-8401