internal medicine patient information forms
advertisement

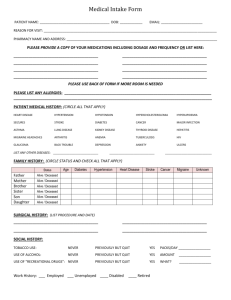
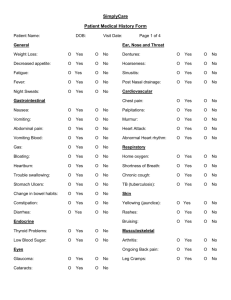
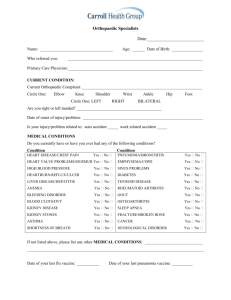
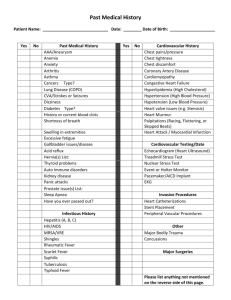
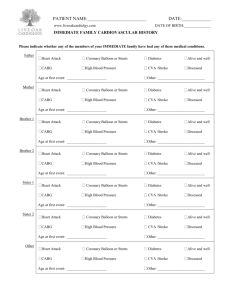
INTERNAL MEDICINE PATIENT INFORMATION FORMS Your Name: ________________________________________ Age: _______ Birthday: ________________ Date: ______________________ Marital Status: _______________ # Children: __________ Do you have a LIVING WILL or ADVANCE DIRECTIVES? Yes/No Allergies to medications: (please list medication and reaction) __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ List present medications: Name: Strength: How often: __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ Do you have or have ever had any of the following: Breathing problems or asthma Yes No Stroke Yes No Diabetes Yes No Tuberculosis Yes No High Blood Pressure Yes No Liver Yes No Arthritis Yes No Tumor or Cancer Yes No Heart problems Yes No Hormonal Problems Yes No Ankle swelling Yes No Steroids Yes No Anticoagulants Yes No Seizures Yes No Digestive problems or ulcers Yes No Smoker Yes No Kidney problems Yes No Use of alcohol Yes No Genital or urinary problems Yes No Anemia Yes No Other: ____________________________________________________________________________________ Please turn over to complete Pg. 2 If Yes to any of the above, please detail: ________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ What other physicians have you seen?___________________________________________________________ Have you ever been hospitalized? (Include date and purpose) ________________________________________ _________________________________________________________________________________________ Family History: Father: Present age or age at Death ___________ If deceased cause of death __________________________ Circle One: Heart Attack Cholesterol problems Stroke/TIA Cancer ________________________________ Hypertension Diabetes Alcoholism Other __________________________________________ Mother: Present age or age at Death ___________ If deceased cause of death __________________________ Circle One: Heart Attack Cholesterol problems Stroke/TIA Cancer ________________________________ Hypertension Diabetes Alcoholism Other __________________________________________ Siblings: Present age or age at Death ___________ If deceased cause of death _________________________ Circle One: Heart Attack Cholesterol problems Stroke/TIA Cancer ________________________________ Hypertension Diabetes Alcoholism Other __________________________________________ Grandparents: Present age or age at Death _______ If deceased cause of death ________________________ Circle One: Heart Attack Cholesterol problems Stroke/TIA Cancer ________________________________ Hypertension Diabetes Alcoholism Other __________________________________________ Children: Present age or age at Death ________ If deceased cause of death ____________________________ Other __________________________________________ What is your occupation? _____________________________________________________________________ What type of hobbies do you enjoy? ____________________________________________________________ __________________________________________________________________________________________ How much exercise do you get a week and what type? _____________________________________________ _________________________________________________________________________________________ Signature: _____________________________________________ (Thank You for completing this form)