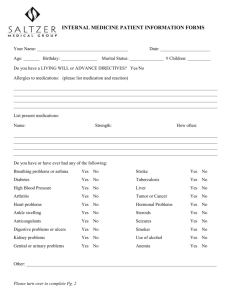
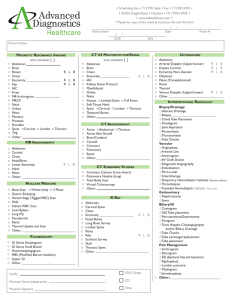
Past Medical History
advertisement

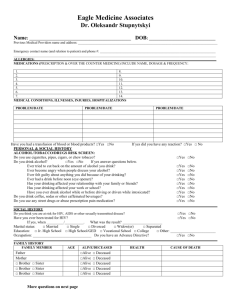
Past Medical History Patient Name: _____________________________ Date: ________ Date of Birth: ____________________ Yes No Past Medical History AAA/Aneurysm Anemia Anxiety Arthritis Asthma Cancers Type? Lung Disease (COPD) CVA/Strokes or Seizures Dizziness Diabetes Type? History or current blood clots Shortness of breath Swelling in extremities Excessive fatigue Gallbladder issues/disease Acid reflux Hernia(s) List: Thyroid problems Auto Immune disorders Kidney disease Panic attacks Prostate issue(s) List: Sleep Apnea Have you ever passed out? Infectious History Hepatitis (A, B, C) HIV/AIDS MRSA/VRE Shingles Rheumatic Fever Scarlet Fever Syphilis Tuberculosis Typhoid Fever Yes No Cardiovascular History Chest pains/pressure Chest tightness Chest discomfort Coronary Artery Disease Cardiomyopathy Congestive Heart Failure Hyperlipidemia (High Cholesterol) Hypertension (High Blood Pressure) Hypotension (Low Blood Pressure) Heart valve issues (e.g. Stenosis) Heart Murmur Palpitations (Racing, Fluttering, or Skipped Beats) Heart Attack / Myocardial Infarction Cardiovascular Testing/Date Echocardiogram (Heart Ultrasound) Treadmill Stress Test Nuclear Stress Test Event or Holter Monitor Pacemaker/AICD Implant EKG Invasive Procedures Heart Catheterizations Stent Placement Peripheral Vascular Procedures Other Major Bodily Trauma Concussions Major Surgeries Please list anything not mentioned on the reverse side of this page. Page 2 Patient Name: ____________________________________________ Date of Birth: __________ Risk Factor Screening Have you ever smoked/used tobacco? If so, how often? Do you still smoke? Do you exercise? If so, how often? Yes No Are you on a special diet? Do you drink coffee? Do you drink tea? Do you drink soda? Do you consume other caffeinated products? If so, what are they? Are you post-menopausal? Have you ever used drugs or Marijuana? If so, what type? Family History Details Do you drink alcohol? If so, how often? Have they ever had heart problems/disease, stroke, diabetes, cancers, high cholesterol or high blood pressure? If so, please specify. Father Is your father deceased? Mother Is your mother deceased? Brothers (collectively) How many? Deceased? Sisters (collectively) How many? Deceased? Allergies List of Medications Reaction? Dose How many times per day? Are you allergic to any medications? If so, please list them below. __________________________________________________________________________________________ __________________________________________________________________________________________