GSH Neonatal TPN Guide
advertisement

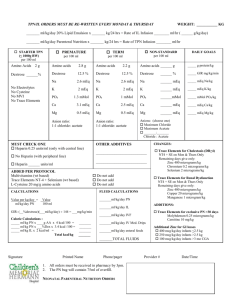
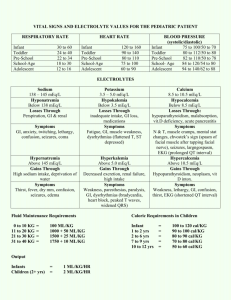
NEONATAL TPN GUIDE PURPOSE: To provide pharmacists a guide for the formulation of Total Parenteral Nutrition (TPN) in neonates PROCESS: Use birth weight of the neonate for the first 8 days, then may switch to actual weight Birth weight needs to be added as “order-specific” in Epic, otherwise the component calculations will default to the daily weight entered by the RN Call SCN and clarify the total fluids and enteral feeds for the day. This will help in verifying the final volume of the TPN COMPONENTS: 1. Fluids: Neonatal TPNs will be started at 80 mL/kg/day Increase daily by 20 mL/kg/day to a max of 150 mL/kg/day TPNs will be written to fulfill the neonate’s estimated TPN needs (according to the estimated advancement of enteral feeds) TPN rate of infusion will be adjusted by the RN to accommodate enteral feeds when the TPN is administered D/C TPN once enteral feeds reach 130 mL/kg/day 2. Dextrose: Initiate TPNs with Dextrose 12.5% for both central and peripheral TPNs Peripheral lines may require Dextrose 10% depending on final osmolality of TPN Central lines may contain up to 20% dextrose Increase or decrease dextrose concentrations for specific situations (i.e. higher concentrations for fluid restricted infants or those with low BGs, lower concentrations for infants with high BGs indicating glucose intolerance) 3. Amino Acids: Preterm infants: trophamine 3.5 g/kg/day and maintain Term infants: trophamine 3 gm/kg/day If infant is feeding, pharmacy will automatically cap the trophamine content to 3.5% Weans IV protein in favor of enteral protein Infants with renal failure and/or high BUN values >80 may require adjustment down 4. Lipids: Initiate lipids at 1.5 g/kg/day. Increase by 0.5 g/kg/day to a MAX of 2.5 g/kg/day Decrease lipids to 1.5 g/kg/day when infant reaches 80 mL/kg/day of enteral feeds If triglyceride level >200, decrease lipids by 50% D/C lipids once enteral feeds reach 100 mL/kg/day 5. Electrolytes and Additives: A. Sodium Initiate with 10-30 mEq/L. Adjust by 10-20 mEq/L/day as needed per Na level. Replace with acetate, chloride, or phosphate depending on lab values. Typically will see 20 mEq/L sodium phosphate in initial TPN (PO4 usually low at birth) MAX sodium in TPN should be ½ NS (77 mEq/L) (may be higher in very few cases) GSH Pharmacy Services Last Updated 08/2015 B. Potassium Initiate with 10-40 mEq/L. Adjust by 10-20 mEq/L/day as needed per K level. Replace with chloride or acetate salts C. Phosphate 20 mEq/L of sodium phosphate typically ordered in initial TPN Phosphate is usually low at birth and requires supplementation Potassium phosphate is less favored due to aluminum contamination of the product D. Magnesium Verify if “mom” was given magnesium prior to delivery If mom received magnesium, do not place in TPN initially If mom did not receive magnesium 2 mEq/L if Mg > 2 4 mEq/L if Mg < 2 E. Calcium Place in central line preferably Preterm infants: 15 mEq/L Term infants: 7.5 mEq/L Adjust per labs up to 20 mEq/L MAX Okay to have 20 mEq/L ordered in initial TPN (this is very typical) F. Multivitamin 2 mL/kg/day to a MAX of 5 mL total volume G. Trace Elements 0.2 mL/kg H. Zinc Note: 200 mcg is contained in Trace Elements Preterm infant or <3 kg: 400 mcg/kg/day (add additional 200 mcg than what is in trace) Term infant or >3 kg: 200 mcg/kg/day I. Cysteine 80 mg/kg/day J. Levocarnitine 10 mg/kg/day K. Heparin 1 unit/mL L. Selenium 3 mcg/kg/day M. Ranitidine 2-4 mg/kg/day ONLY if GI issues identified 6. Daily Labs Order daily NCMPL –Contains special pre-term and post-term ranges for PO4 and ageappropriate reference ranges and panic values for sodium and potassium. Includes the basic constituents in CMPL as well as Mag and PO4 Requires 0.6 mL whole blood in green (preferred) or gold microtainer GSH Pharmacy Services Last Updated 08/2015