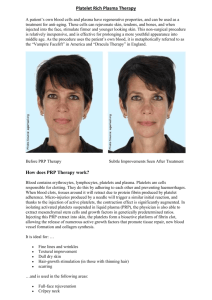
Platelet Rich Plasma
advertisement

Platelet Rich Plasma (AAOS 2011) Background Information -Platelets derived from whole blood using simple cell-separating systems provide a release of various growth factors that participate in tissue repair processes. -The normal platelet count is 150,000-350,000 per ml of blood. Platelets are produced in the bone marrow, the same as the red cells and most of the white blood cells. Platelets are produced from very large bone marrow cells called megakaryocytes. As megakaryocytes develop into giant cells, they undergo a process of fragmentation that results in the release of over 1,000 platelets per megakaryocyte. The dominant hormone controlling megakaryocyte development is thrombopoietin (often abbreviated as TPO). -The average lifespan of a platelet is normally just 5 to 9 days. Platelets play a fundamental role in hemostasis and are a natural source of growth factors. They circulate in the blood of mammals and are involved in hemostasis, leading to the formation of blood clots. Platelets contain alpha and dense granules. Activated platelets excrete the contents of these granules into their canalicular systems and into surrounding blood. -There are three types of granules: ▪ Dense (or delta) granules (containing ADP or ATP, calcium, and serotonin) ▪ Lambda granules - similar to lysosomes and contain several hydrolytic enzymes. ▪ Alpha granules (containing platelet factor 4, transforming growth factor-β1, platelet-derived growth factor, fibronectin, B-thromboglobulin, vWF, fibrinogen, and coagulation factors V and XIII). -Platelets contain 1,100 bioactive molecules. Plasma contains important proteins as well (hence Platelet rich Plasma). Clotting is prevented by chelating calcium. -PRP preparations vary in regards to: 1) 2) 3) 4) Amount of blood needed Presence (or absence) of WBC Activation of thrombin Platelet recovery -Some may claim “more platelets” but they are really just collecting more blood so you need to know the concentration. -Castillo et al (AJSM 2011: 266-71): The GPS III and Magellan concentrate leukocyterich PRP, which results in increased concentrations of WBCs, PDGF-αβ, PDGF-ββ, and VEGF as compared with the leukocyte-poor PRP from Cascade. Overall, there was no significant difference among systems in the platelet concentration, red blood cell, active TGF-β1, or fibrinogen levels. There was a lot of variability between systems. -Each centrifuge is set up for the specific system being used. Do not mix and match centrifuges, because this will alter the recovery of the platelets (each centrifuge is optimized for each system). -More PRP does not mean “better”. There is an inhibitory level of PRP (just think of negative feedback loops) but we don’t know what levels are good, further research is needed. -Thomopolous showed that combining growth factors is important. Also proper ratios of growth factors is important and the wrong ratio can lead to scar as opposed to good tendon. -Described uses of PRP: 1. Rotator Cuff Repair 2. Lateral Epicondylitis 3. Achilles Tendinopathy -Among patients with chronic Achilles tendinopathy who were treated with eccentric exercises, a PRP injection compared with a saline injection did not result in greater improvement in pain and activity. 4. Patellar tendonitis 5. Muscle Strain (Hamstring, Gastrocnemius, Achilles) 6. Ligament Injury (MCL, ACL) 7. Osteotomy sites 8. Spine Fusion 9. Meniscus Repair 10. Plantar Fascitis 11. Osteoarthritis of the Knee 12. Venous stasis ulcers 13. Dental work (original description)