BGA_-_For_Patients_files/BGA Patient Information
advertisement

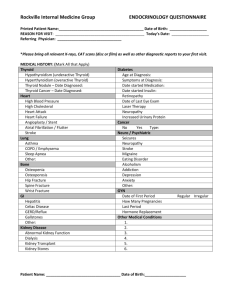
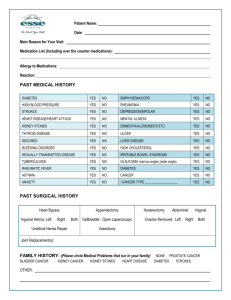
Patient Information Binghamton Gastroenterology Associates Name: ________________________________Today's Date: ________________DOB: ____________ Age:_____ Employer: Occupation: How where you referred to our office? What is the main reason for your visit today? PATIENT MEDICAL HISTORY Have you had any of the following problems or conditions? Please circle Yes or No Liver Disease Y N Diabetes Y N Thyroid Disorders Y N Hepatitis Y N Asthma Y N High Blood Pressure Y N Heart Disease Y N Cancer Y N Heart Murmur Y N Heart Attack Y N Arthritis Y N Prostate Problems Y N Angina Y N Seizures Y N Colon/Bowel troubles Y N Eye Disorders Y N Clotting Disorders Y N Kidney Disease Y N Tuberculosis Y N Depression Y N Stomach Ulcers Y N Rectal Trouble Y N Heart Arrhythmia Y N Infectious Disease Y N Emphysema Y N Radiation Y N Sleep Apnea Y N Anxiety Y N Psychiatric Illness Y N Other Y N If yes to any of the above, please explain SURGICAL HISTORY (Place a check mark next to any of the following surgeries you’ve had) Heart Kidney Breast Biopsy Tonsils Uterus/ Ovaries Mastectomy Appendix Hysterectomy Colon/Intestines Gallbladder Stomach/Hernia Prostate Cataract Vascular Thyroid Joint Replacement OTHER HOSPITALIZATIONS/SURGERIES (Please list reasons and year) FAMILY HISTORY (BLOOD RELATIVES ONLY) Circle Yes or No and specify relationship Cancer Y N Kidney Disease Y N Thyroid Disorders Y N Liver Disease Y N Lung Disease Y N High Blood Pressure Y N Pancreatic Disease Y N Heart Disease Y N Arthritis Y N Blood Disorders N Diabetes Y N Bowel Disorders Y N Anesthesia Reaction Y N Y CONTINUED ON THE BACK SOCIAL HISTORY: Marital Status: S M D W Do you Smoke? ________________ If Yes how much? __________ Would you like information on quitting? Y Do you drink Alcohol? _____________ If Yes how much? _______ Do you have a Health Care Proxy? Have you received the Pneumonia Vaccine? Y N Y N N If yes, when If you are between the ages of 45-65 have you been tested for Hepatitis C? Y N If yes, result List any Allergies to drugs, environment, food, etc. REVIEW OF SYSTEMS: Do you have any of the following problems or conditions? Circle Yes or No Constitutional Respiratory Integumentary Fatigue Y N Frequent Cough Y N Rashes Y N Weight loss Y N Wheezing Y N Sores Y N Weight gain Y N Shortness of Breath Y N Hair Loss Y N Fever Y N Gastrointestinal Night sweats Y N Abdominal Pain Y N Headaches Y N Appetite Problem Y N Tremors Y N Eyes Neurological Blurred vision Y N Nausea/Vomiting Y N Dizzy Spells Y N Double vision Y N Indigestion/Heartburn Y N Numbness/Tingling Y N Pain Y N Change in Bowel Habits Y N Seizures Y N Glasses? Y N Genitourinary Ear/Nose/Throat/Mouth Psychological Urinary Frequency Y N Mood Swings Y N Hearing Loss Y N Painful Urination Y N Depression Y N Nasal/Sinus Problems Y N Nighttime Urination Y N Other Y N Sore/Bleeding Gums Y N Hesitant Stream Y N Endocrine Dentures? Y N Musculoskeletal Heat Intolerance Y N Cardiovascular Leg Pain Y N Cold Intolerance Y N High Blood Pressure Y N Muscle Weakness Y N Excessive Sweating Y N Chest Pain Y N Back Pain Y N Excessive Thirst Y N Leg Swelling Y N Movement Limitation Y N Palpitations Y N Hematologic/Lymphatic Swollen Glands Y N Spontaneous Bleeding Y N Bruise Easily Y N Blood Clotting Y N