Appendix D - Self Certification Form (Operational Staff)
advertisement
")
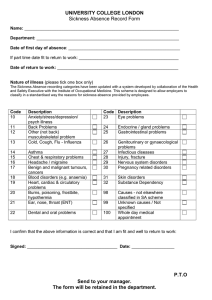
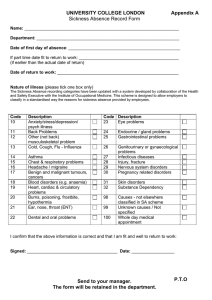
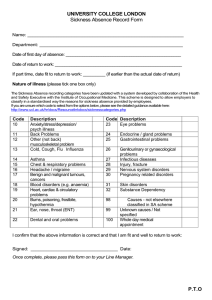
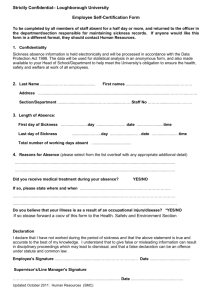
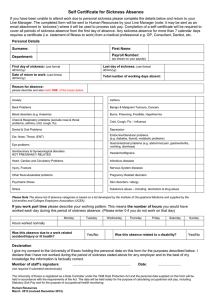
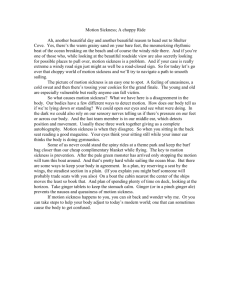
Appendix B SELF CERTIFICATION FORM (SCF1A) PERSONAL DETAILS Name: School / Department: National Insurance Number: PERIOD OF SICKNESS ABSENCE Date absence began: Last date of absence: Date of return to work: REASONS FOR ABSENCE Please tick all that are applicable and provide brief description below Anxiety / Depression/Other Mental Health Condition Asthma Back Problems Benign and Malignant Tumours / Cancers Blood disorders (e.g. anaemia) Burns/poisoning / frostbite / hypothermia Chest & respiratory problems – excluding nose & throat/asthma/cold/cough/flu Cold/cough/influenza Dental and oral problems Ear / nose / throat (ENT) Endocrine / glandular problems (e.g. Diabetes / thyroid / metabolic problems) Eye problems Gastrointestinal Problems (e.g. abdominal pain / vomiting / diarrhoea) Genitourinary & gynaecological disorders – excluding pregnancy related disorders Headache / migraine Heart / cardiac / circulatory problems Injury / Fracture Nervous system diseases (e.g. Multiple Sclerosis / Cerebral Palsy / Epilepsy) Other Musculoskeletal Problems (not back) Pregnancy related disorders Page 1 of 2 July 2015 Skin disorders Stress Infectious disease – hand foot and mouth / malaria / meningitis / measles / mumps / shingles Substance misuse – Including alcoholism & drug abuse Substance misuse – Including alcoholism & drug abuse Details of sickness absence: ..…………………………………………………………………………….………………………….... …………………………………………………………………………………………………………… I declare that I have not worked during the above period of sickness and that the information given is correct. Signed: ………………………………………………….. Date: ………………………….. Please pass this form to your manager for discussion at a return to work meeting. Manager: I confirm that I have met with the above named to discuss this period of sickness. Signed: ………………………………………………….. Page 2 of 2 Date: ………………………….. July 2015