Specialist Diabetes Referral Form - Gloucestershire Hospitals NHS
advertisement

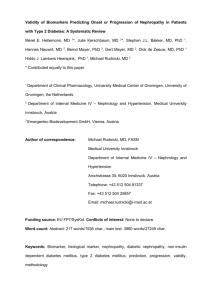
GLOUCESTERSHIRE HOSPITALS NHSFT SPECIALIST DIABETES REFERRAL FORM Patient Details SURNAME FIRST NAME ADDRESS NHS NUMBER TELEPHONE NUMBER DATE OF BIRTH REFERRED BY GP NAME & TEL PRACTICE NAME GP FAX NUMBER ETHNICITY ENGLISH SPOKEN Exclusion Criteria: 1. Not registered with a Gloucestershire GP 2. Stable/non-complex T2 Please tick reason for referral Assessment/management of Specialist nephropathy (incl. those on dialysis) those on Insulin Pump Therapy Specialist diabetic footcare Specialist antenatal diabetes care (women with diabetes contemplating pregnancy or who are pregnant) Type 1 diabetes for: 1)children Other reason for referral – e.g. significant or worsening (incl. transition) and 2) those complications requiring acute/specialist input (please with poor blood glucose control provide information below) Investigations / Bloods HbA1c Total cholesterol eGFR HDL ACR LDL Other Significant Information BMI Weight Serum albumin ALT Alkaline phosphatase BP Macro and Micro Vascular Complications Myocardial infarction or angina Retinopathy Coronary artery bypass grafts Neuropathy AAA Erectile dysfunction Stroke Nephropathy Other Conditions - please tick below to indicate co-morbidity Thyroid dysfunction Other Anaemia Dementia Asthma / Chronic obstructive pulmonary disease Mobility problems* Mental health or LD disorders* Other specialist services* Housebound None *PLEASE INCLUDE DETAILS IN REASON FOR REFERRAL OVERLEAF Review date: February 2016 Reason for referral: Please note that both the GCS Community Diabetes Team and GHFT Diabetes & Endocrinology Advice & Guidance remain an option for those patients who do not fulfil the above criteria but maybe considered complex due to intercurrent illnesses or ther complicating factors; this may still result in a referral to the hospital specialist team PLEASE ATTACH SUMMARY SHEET WITH PMH AND CURRENT REPEAT MEDICATION Review date: February 2016