billconnell_148_20130611072244
advertisement

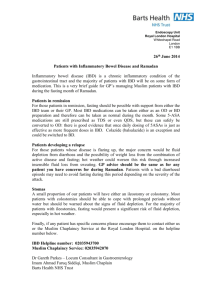
Cost savings associated with IBD nurse-coordinated anti TNF therapy for Crohn’s disease at a suburban Melbourne hospital Background: The equitable implementation of expert, integrated, patient-centred care for inflammatory bowel disease (IBD) patients is a major challenge to governments, insurers and health care organisations. In larger centres, multidisciplinary services provide superior care for patients with chronic complicated disease phenotypes, but this option is usually unavailable in smaller or regional centres. Alternatively, specialist IBD nurses working cooperatively with individual specialists or via telemedicine can facilitate high-quality, local IBD care in regional areas. We have reviewed the clinical outcome of IBD nurse-coordinated anti TNF therapy at a suburban Melbourne hospital. Methods Since 2008, anti-TNF therapy has been available for Crohn’s disease (CD) patients attending at Werribee Mercy Hospital, a suburban centre servicing the City of Wyndham (population of 160,000). In 2011, a dedicated fortnightly IBD clinical outpatient service staffed by a single gastroenterologist was established, and patients requiring anti-TNF therapy for Crohn’s disease had their care co-ordinated by an IBD nurse. Hospital admission rates, corticosteroid usage, mucosal healing and need for surgery were reviewed before and after anti TNF therapy was started. Results: 21 CD patients were treated with anti TNF therapy. Median disease duration was 6 years (range 1-17 years) prior to therapy and 4 years (range 1-5 yrs) after commencement of therapy. Before treatment, all 21 patients had endoscopic evidence of active mucosal inflammation and required corticosteroids. Before treatment, 8 patients had undergone 11 intestinal resections, 5 required repeated perineal surgery and 14 had been admitted on 23 occasions for medical management of their disease. After treatment, one patient required a further intestinal resection and drainage of a perianal abscess, another underwent laparoscopy for adhesive small bowel resection, and one was medically treated for a small bowel obstruction. After treatment, complete mucosal healing was achieved in 14/19 patients who had a follow up colonoscopy, and 2 have needed further courses of corticosteroids. Five women have had 8 successful pregnancies on anti TNF therapy, and all but two patients electing to work were fully employed. Conclusion: Although this series is small, the preliminary experience of anti TNF therapy for CD highlights a dramatic reduction in health care utilization (need for surgery, medical admissions), corticosteroid usage and disease activity (endoscopic remission). Improvement in personal quality of life is difficult to measure retrospectively, but the capacity for full time employment and fecundity are notable beneficial endpoints. Attending to administrative requirements and safety monitoring regarding anti TNF therapy is detailed, intensive and time-consuming. These indirect elements of care are best co-ordinated by an IBD nurse. For individual hospitals and State Governments, the upfront cost associated with employing IBD nurses is clearly offset by considerable savings resulting from reduced admissions and need for surgery.