Supplemental Materials - JACC: Cardiovascular Imaging
advertisement

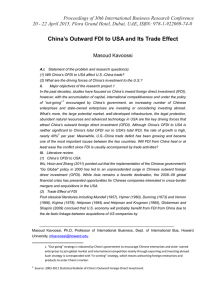
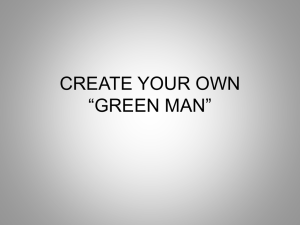
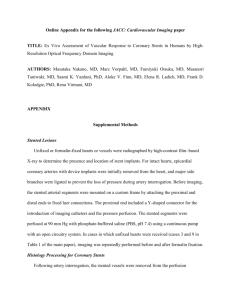
Supplemental Materials 1 Supplemental Figure 1. Partitioning analysis for IB-IVUS for IB-IVUS-derived TCFA based on histologic identification of TCFA. We sought to define TCFA based on IB-IVUS measurements by recursive partitioning analysis (RPA) which is an exploratory multivariate method known as classification tree, allowing identification of candidate variables in distinguishing subgroups, free of distributional and linearity assumption. Among 360 plaques (18 TCFA and 342 non-TCFA on histology), RPA firstly split the groups by % lipid area with a threshold of 32.3%, with the subgroup <32.3% lipid area having no TCFA. Secondly, RPA split the subgroup >32.3% lipid area into two with a threshold of 65.1% lipid area, with the subgroup >65.1% lipid area consisting of 3 TCFA and 0 non-TCFA. Then, RPA chose a threshold of 10.5mm2 in plaque area to best separate the subgroup of % lipid area >32.3 but <65.1%. Subsequently, RPA chose a threshold of 72% in plaque burden as the parameter to separate the subgroup with plaque area >10.5%. However, we did not adopt this third parameter because of the limited number of TCFA (18) in our cohort. Utilizing 2 variables derived from the exploratory analysis shown as above, finally we defined IB-IVUS-derived TCFA as (i) cross-sectional % lipid area >65.1% or (ii) % lipid area >32.3 but <65.1% and plaque area >10.5mm2. Abbreviations: IB-IVUS, integrated backscatter intravascular ultrasound; RPA, recursive partitioning analysis; TCFA, thin cap fibroatheroma 2 Supplemental Figure 2. Representative OFDI images co-registered to histology Left column: cross-sectional histologic images of coronary plaques. Mid column: high powered images of inset box in the left column. Right column: OFDI images co-registered to histology. Fibrous intima (upper row) appears to be homogeneous bright signals in OFDI. Lipid pool (mid row) appears to be dark area without clear border. Macrophages (Mø) are seen infiltrating into the plaque. Sheet of calcium (lower row) appears to be solid black area with clear border. 3 Supplemental Figure 3. Fibrocalcific plaque misdiagnosed as lipid-rich by OFDI Left: cross-sectional histology of fibrocalcific plaque. A large sheet of calcium is present extending into the deeper regions of the plaque near the media. In the mid column are highpower images of the boxes inset in the left image. Sheet of calcium (Ca++) and macrophage (Mø) infiltration (red arrowheads) are seen. Right: corresponding image of OFDI. Sheet of calium is present deep in the plaque is less clear on OFDI as the margins are poorly delineated. 4 Supplemental Figure 4. TCFA missed by OFDI Left: cross-sectional histology of a TCFA with a small area of necrosis (NC). Middle image is a high power of the box inserted in the left image. Fibrous cap covering the NC is thin <65 µm. Right: corresponding image of OFDI. OFDI readers missed the regions of the thin fibrous cap (white arrowhead). 5 Supplemental Figure 5. Diagram of pseudo or true OFDI-derived TCFA In OFDI, macrophages appear high intensity signals with trailing shadow. It is difficult to correctly diagnose tissues behind macrophages. Abbreviations: OFDI, optical frequency domain imaging; PIT, pathologic intimal thickening; TCFA, thin cap fibroatheroma; Th-FA, thick fibroatheroma. 6 Supplemental Table 1. IB-IVUS measurement of coronary plaque IB-IVUS measurement Histology IEL area (mm2) Lumen area (mm2) Plaque area (mm2) AIT/Fib 8.9 (6.8, 10.6) 5.9 (4.4, 7.2) 2.6 (2.0, 4.0) 31.9 (24.6, 40.7) 2.8 (1.4, 5.1) 18.0 (13.2, 22.7) 65.7 (60.6, 70.1) 10.6 (7.5, 16.8) PIT 11.7 (8.4, 15.1) 5.7 (4.2, 8.4) 5.4 (4.0, 7.5) 47.8 (39.9, 54.7) 1.7 (0.9, 3.1) 12.5 (8.6, 16.8) 62.1 (57.4, 66.7) 22.0 (14.4, 30.1) Th-FA 13.4 (10.1, 18.7) 4.2 (2.9, 7.8) 8.7 (6.9, 11.2) 66.6 (52.4, 73.7) 2.1 (0.8, 4.3) 10.5 (7.4, 14.5) 53.5 (42.9, 61.1) 32.3 (22.4, 43.0) TCFA 17.2 (10.0, 21.2) 5.7 (2.8, 10.4) 10.6 (8.0, 12.5) 63.8 (49.9, 78.5) 1.1 (0.4, 2.1) 6.6 (3.7, 9.6) 44.6 (34.8, 50.8) 46.8 (39.7, 55.7) Fibrocalc 10.9 (8.4, 14.1) 4.2 (2.8, 5.7) 7.3 (5.2, 9.2) 61.9 (50.9, 67.6) 10.8 (6.5, 14.3) 19.6 (13.2, 22.5) 53.6 (46.8, 58.2) 15.2 (10.9, 23.3) <0.001 0.002 <0.001 <0.001 <0.001 <0.001 P value Plaque burden (%) <0.001 % Calc % Dense fib % Fib % Lipid <.0.001 Values of IB-IVUS measurements are expressed as median (interquartile). Abbreviations: AIT, adaptive intimal thickening; IB-IVUS, integrated backscatter intravascular ultrasound; IEL, internal elastic lamina; Fib, fibrous plaque; Fibrocalc, fibrocalcific plaque; PIT, pathologic intimal thickening; TCFA, thin cap fibroatheroma; Th FA, thick cap fibroatheroma. 7 Supplemental Table 2. Positive predictive values of OFDI/IB-IVUS for the detection of vulnerable plaque TCFA detection Positive predictive value *95% confidence interval Both by OFDI and IB-IVUS 100.0% 69.2 - 100.0% Only by OFDI (non-TCFA by IB-IVUS) 30.8% 9.1 - 61.4% Only by IB-IVUS (non-TCFA by OFDI) 14.3% 1.8 - 42.8% Neither by OFDI nor IB-IVUS 0.6% 0.1 - 1.9% * 95% confidence interval of nominal variables were calculated by exact binomial probabilities. Abbreviations: IB-IVUS, integrated backscatter intravascular ultrasound; OFDI, optical frequency domain imaging; TCFA, thin cap fibroatheroma 8 Supplemental methods Histology Processing for Coronary Arteries Following intravascular imaging, the hearts were perfusion-fixed with 10% buffered formalin via the coronary arteries for at least 20 to 30 minutes. Following in situ perfusion of the coronary arteries, imaged epicardial coronary arteries were removed from the heart and radiographed. If on radiography calcification was prevalent the vessels were decalcified with EDTA using a microwave processor. The coronary arteries were segmented at 3 cm intervals, placed in tissue cassettes and processed through ethanols and xylenes for dehydration. The samples were further segmented at 3 mm intervals and embedded in a single paraffin block maintaining proximal and distal orientation. The 1st two slides from each block were stained with hematoxylin-eosin (H&E) and modified Movat pentachrome stains. Reproducibility for IB-IVUS measurements The reproducibility of IB-IVUS measurements was evaluated by Spearman rank correction coefficient model. To evaluate the intra- and inter-observer agreements, 50 of 360 coronary sections were randomly selected, in which IB-IVUS measurement was performed. The p values for correlations of all parameters, including the lumen area, were <0.01 for both the intra- and inter-observer agreement. Therefore, the IB-IVUS reproducibility is less likely affected by the lumen contour. 9