Pain Medications in ED patients
advertisement

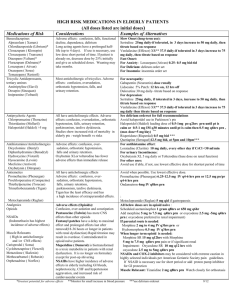
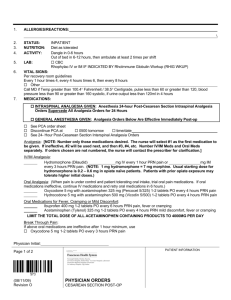
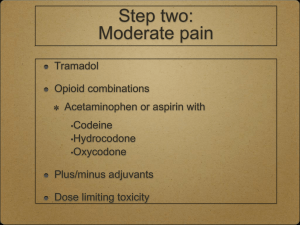
Pain Treatment for Senior ED Patients General Guidelines Parenteral medications in ED: Morphine 2 mg to 4 mg IV or SQ prn OR Hydromorphone 0.5 mg IV or SQ prn Oral medications in ED or for outpatient management: Scheduled Acetaminophen 1 gram q8hrs or 650 mg q6hr PLUS Oxycodone 2.5 mg -5 mg PO Q 3-4 hours prn OR Morphine 7.5 mg PO Q 3-4 hours prn Notes: Doses of opioids are for opioid naïve patients. Contact pharmacist for dosing patients on chronic opioid therapy. IV medications can be repeated as frequently as q15”, SQ medications q30”. Oxycodone preferred over morphine in renal impairment. If patient’s pain is due to a fall: Consider addition of Vitamin D and a recommendation for a Vitamin D level as an outpatient: OsCal 500 with D plus Vitamin D 400 units daily (800 units total per day reduces falls risk by 20%). Medications to Avoid Tricyclic Antidepressants Amitriptyline (Elavil) Imipramine (Tofranil) Doxepin (Sinequan) High anticholinergic effects: Can cause delirium, falls, constipation, urinary retention. Muscle Relaxants Carisprodal ( Soma) Methocarbamol ( Robaxin) Cyclobenzaprine ( Flexeril) Metazolone ( Skelexin) Orphenadrine ( Norflex) Sedating, some have anticholinergic effects, increased risk of falls, delirium, constipation, urinary retention. NSAIDs Indomethacin has highest incidence of adverse effects Certain Opioids Pentazocine (Talwin): more CNS effects than other opioids. Fentanyl patch: delay to maximal effect, prolonged effects after removal, rapid titration may cause overdose, contraindicated in opioid naïve patients. Meperidine (Demerol): toxic metabolite in patients with renal dysfunction, use restricted to certain indications at SHS. Alternatives For Neuropathic Pain: If CrCl > 50 ml/min: Gabapentin (Neurontin) – 300 mg at bedtime x 1 day, then 300 mg BID x 1 day, then 300 mg TID; If CrCl < 50 ml/min, check drug reference for dosing. Lidocaine 5% Patch - 12 hrs on, 12 hrs off Duloxetine (Cymbalta) 30 mg daily, may increase to 60mg daily in 1 week based on response. Nortriptyline 10 mg at bedtime (has some anticholinergic effects) Opioid, acetaminophen combination Tizanidine (Zanaflex) 2 mg q8hrs prn. Not recommended in patients prone to orthostasis. Opioid, acetaminophen combination NSAIDs and COX-2 inhibitors may be considered with extreme caution in highly selected individuals per American Geriatric Society Pain Guidelines. If an NSAID is prescribed, add a proton pump inhibitor or misoprostol for GI protection. For Long-term Pain Relief: Morphine SR 15 mg q12hrs Plus Morphine 7.5 mg PO Q 3-4 hours prn Or if significant renal Impairment Oxycodone SR 10 mg q12hrs Plus Oxycodone 2.5 mg to 5 mg q4hrs prn Adapted from: J Am Geriatr Soc 2010; 58: 1299-1310; BMJ 2009; 339:b3692; JAMA 2004;291:1999-2006.