Click here to file Ortho
advertisement

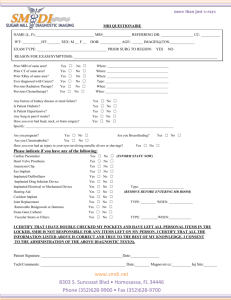
__________________________________ Ortho-tag RFID Touch Probe System for a National Total Joint Registry By J. Lee Berger, MD; Marlin Mickle, PhD Investigation performed at the RFID Center of Excellence University of Pittsburgh ABSTRACT Knowledge of the technical characteristics of implanted medical devices and surrounding tissue is very important for patients, treating physicians and manufacturers to ensure patient safety and quality control. However, one of the major technical problems in accomplishing this is the inability to obtain information regarding the implant itself and the surrounding environment without using invasive methods. The metallic total joint implant present a classical RFID barrier for reading a tag, and human tissue is a difficult medium for propagating RF energy. Both of these issues are overcome by technology we have developed at the RFID Center of Excellence at the University of Pittsburgh. We have invented a system termed Ortho-tag that provides radiofrequency (RF) tags, attached to hip and knee implants in the human body and uses our patented touch probe device to obtain identifying information about the implant as data stored on the orthotag as well as information about the environment of the surrounding tissue as measured by incorporated biosensors. The information obtained from the Ortho-tag RFID Touch Probe Based system will be beneficial in developing a safe, accurate, secure, simple user friendly system for the identification and monitoring of implanted medical implants that can be incorporated into any type of approved National Joint Registry. Introduction Total joint replacement (TJR) of diseased or disabled knees and hips using artificial implants offers dramatic improvements in functional ability and quality of life to hundreds of thousands of patients each year. TJR represents the largest single category of hospital care (Diagnosis Related Group) for Medicare beneficiaries and is spreading rapidly to younger patients who seek better mobility and less chronic pain than earlier generations (Orthopedics Data Compendium, 2006). Moreover, the age of the general population is increasing, resulting in a need for implants that last longer and are used latter into life. Even for those who don’t already have implants, the aging population adds to the population individuals exhibiting osteoarthritis later in life than previously and, as a consequence increasing the age at which first prostheses are implanted. Further, owing to a more active life style among a portion of the US population, TJR is occurring in younger individuals. Taken together, as illustrated in Table 1, which summarizes data adapted from the National Center for Health Statistics, there has been a rapid growth in the use of hip and knee prostheses. Hip Replacement Total Hip (81.51) 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 117 127 125 124 134 138 144 160 168 152 165 193 220 234 Partial Hip (81.52) 90 88 84 93 97 103 103 112 106 106 119 109 108 * Knee Replacement Revision (81.53) Total Knee (81.54) Revision (81.55) 25 23 26 28 29 30 37 33 30 31 36 43 36 * 160 167 179 209 216 245 259 266 267 299 326 381 418 478 17 13 15 19 18 20 25 23 25 28 29 35 36 * Total 409 418 429 473 494 536 568 597 596 616 675 761 818 712 *Data not available Table 1. Procedure Volumes in the United States – Number of Hip and Knee Replacement Procedures (by ICD-9-CM code) in the U.S. 1991-2004. Numbers are in thousands rounded to the nearest thousand. (Adapted from data from American Academy of Orthopedic Surgeons, Department of Research and Scientific Affairs. Original data from National Hospital Discharge Survey, 1991 – 2004; U.S. Department of Health and Human Services; Centers for Disease Control and Prevention; National Center for Health Statistics) Even more compelling are data summarized by Wilson, et al (2008) showing that the demand for orthopedic implants is forecast to continue to rise. In 2005 approximately 750,000 hip and knee prostheses were implanted in the US, representing a 70 percent increase from the previous 5 years (Wilson, et al, 2008). They estimate that by 2030 the number of hip replacements will more than double while the number of knee replacements will increase 6-fold for a total of almost 4.5 million implants (Wilson, et al, 2008). Using data from the Nationwide Inpatient Sample (NIS) from 1900 to 2003 similar findings have been reported by Kurtz, et al (2007) and subsequently confirmed by others (e.g., Poultsides, et al, 2010). Specifically, using a Poisson regression analysis with age, gender, race and/or ethnicity, census region, and calendar year as covariates to account for differences in prevalence among population subgroups as well as changes over time, Kurtz, et al estimated that the demand for primary total hip arthroplasty will almost double from approximately 209,000 in 2005 to 572,000 hip implants by 2030. Further, they estimated that if the number of total knee arthroplasties continues at the current rate, the demand for primary total knee arthroplasty would grow by nearly 7-fold from 450,000 in 2005 to 3.48 million knee procedures by 2030. While the increase in hip and knee implants will no doubt improve the quality of life for an ever increasing number of individuals, there will be a concomitant increase in the number of revisions required. The major cause of revisions will result from periprosthetic infection, although other causes will contribute to an overall increase in hip and knee implant surgery. Kurtz, et al (2007) estimate that the number of hip revisions will double between 2005 and 2026 (i.e., it will take 21 years) while the same level will be reached for revision of knee implants by 2015, approximately twice as fast (i.e., in 10 years). If the already established trend between 1990 and 2003 continues, total hip arthroplasty revisions are projected to increase by approximately 1.5 times from approximately 41,000 in 2005 to approximately 97,000 in 2030 and total knee arthroplasty revisions were projected to increase by approximately 6-fold from approximately 38,000 in 2005 to approximately 268,000 in 2030. Issues Arising From Increased Hip and Knee Implant Surgery With the growing demand for both original hip and knee arthroplasties, along with the attendant need for implant revisions, there will be an increased concomitant need to monitor the condition of the implant and biological environment in which it exists without using invasive procedures. Among the specific kinds of information needed are (a) manufacturing information about the implant, and (b) patient/implant information normally contained in medical records about the implant surgery (e.g., model of the implant, date of surgery, surgeon) which, themselves, are often not available at the time of the patient visit. State of the biological environment of the implant: Periprosthetic infection (septic joint failure) Deep tissue infection is one of the major causes of revision surgery for total hip and total knee implants. It has been estimated to occur in between 1% and 4% of surgeries (Bozic & Ries, 2005) and is projected to increase between 2005 and 2030 by nearly 14-fold, from 3400 cases to 46,000 cases, for total hip replacement and by approximately 27-fold, from 6400 cases to 175,500 cases, for total knee replacement (Kurtz, et al, 2007). The American Academy of Orthopedic Surgeons (2010) estimates that there is a 1%2% incidence of infection at 2 years post surgery and that it accounts for 25% of knee revisions and 15% of hip revisions (AAOS, 2010). The vectors for infection vary and include bacteria such as S. aureus both in community- and health-care-based settings (Poultisides, et al, 2010). Recently, the AAOS approved and issued evidence-based clinical practice guidelines for the diagnosis of periprosthetic joint infection of the hip and knee (AAOS, 2010). As stated in the AAOS article accompanying the issuance of the guidelines (Parvizi, 2010) the challenge is to correctly diagnose periprosthetic joint infection so that effective treatment regimens capable of eradicating the inciting organism can be prescribed. The chairman of the committee that developed the guidelines, Dr. Craig Della Valle, noted that a diagnosis of septic joint failure can be very difficult to make. The guidelines recommend several procedures, each of which is invasive, including serology, drawing joint fluid, injection of radioisotope for bone scan, and biopsy of tissue to detect acute inflammation and the presence of neutrophils. These diagnostic procedures can cause the patient discomfort and/or pain, and as noted in the report can produce equivocal results requiring repeated administration. Manufacturing information about the implant With the rapid increase in the number of implants to be used in treating osteoarthritic hip and knee joints, manufacturers are increasingly concerned over the production of counterfeit devices sold under the same name as the legitimate one. The use of the Ortho-tag RFID system will provide useful information for manufacturers, physicians and healthcare providers worldwide. Not only will information transmitted from the Ortho-tag be able to identify the manufacturer of a device it could also provide information that would identify a specific individual device. This information could be used to determine whether or not a specific prosthesis is one that is among a group that has been recalled without a need for referring to medical records which, themselves, are not always available. Surgical/arthroplasty implant information Another potential use of RF technology is to carry surgical or arthroplasty information, information that is typically contained in patient records. However, as most physicians know, these records are not always available or complete and patients do not have complete or accurate recall of even simple events (e.g., date of implantation, surgeon completing the implant) that may have taken place many years in the past. It will enhance post-surgical treatment if the surgical/arthroplasty implant information is available with the implant itself. Further, sensors that can monitor the tissue environment surrounding the implant would reduce the reliance on other less direct approaches to diagnosing problems such as infection. The need for a National Total Joint Registry The United States has lead the world in medical technology yet lags behind the European community in registration and accountability of implanted medical devices. There is a need for a universal user-friendly system for identification of implanted medical devices. Suggested paper or web based Total Joint Registries are only as good as the data entry and are fraught with inconsistency and inaccuracy of data collection, data entry and follow-up, We propose in body transcutaneous RFID tag touch probe powered and read system of identification of implanted medical devices. The system named Ortho-tag was invented by the authors; Dr Lee Berger, an orthopedic surgeon and Dr Marlin Mickle, Professor of Bioengineering at the University of Pittsburgh and Director of the RFID Center of Excellence. Our research and inventions have overcome the obstacles of in body radiofrequency transmission and of interference and scatter of radiofrequency signals by metal implants. Concerns of patient confidentiality are addressed and answered by the Ortho-tag Touch Probe in that it must physically contact the individual to read any data from the embedded tag and also is password protected by the patient, healthcare provider and implant manufacturer complying with and exceeding all HIPPA regulations, The system simplifies data and registry collection of implanted medical devices and improves the consistency and accuracy of the data programmed and logged into a computer or web based National Total Joint Registry. This type of collection system is easy to use and cost effective for manufacturers, physicians, hospitals and the healthcare system. From a medical legal aspect it improves the accountability of implanted medical devices and supplies prima fascia evidence of the characteristics of the implant and the programmed information in the Ortho-tag. The performance of orthopaedic implants is traditonally studied by three types of formats: prospective randomized clinical trials; meta-analysis; and retospective studies. In order to perform these types of studies it requires considerable effort and the publication of results can take months or years after the data has been collected. Surgeons and hospital personal have limited time, limited desire and limited focus in filling out paper forms and questionairs or reviewing patient and hospital records to obtain retrospective information about medical devices and their performance and patient clinical short and long term results. To address this situation and provide for centralized documentation of information an “International Documentation and Evaluation System” database was created by more than fifty participating hospitals from counties including Switzerland, Germany, France, Italy, Belgium, Australia and Canada. This database has been in existence for over forty years and has and continues to provide important information about primary and revision total hip and total knee implants. Dr. M.E. Muller and his colleagues at the University of Bern, Switzerland provided much of the information in the database. In Sweden, a National Hip and Knee Registry has been in effect for many years and has set a standard for data collection and is a valuable tool for research studies in that country and worldwide. In the United States, William Mahoney, MD stated that a National Joint Registry would be beneficial to avoid the problems of data collection and long delays for the results of in clinical trials, metaanalysis and retrospective review of data. Three goals as proposed by Mahoney included the definition of the patient population in the epidemiology of patients receiving total joint replacement; the gathering of data for outcome studies on total joint replacement, data that would be helpful to identify risk factors in total joint replacement and the accumulation of continuous information from the national registry databank for up to the minute feedback that can be used by surgeons, healthcare providers and manufacturers to improve patient care. In recent years there has been considerable interest and discussion by implant manufacturers, surgeons, healthcare providers, the United States National Institute of Health, the American Association of Orthopaedic Surgeons, and respective Hip and Knee Societies in developing the framework and guidelines for a National Joint Registry. This is a considerable task with practical scientific, logistical and legal concerns. Practical considerations include establishing a universal system of implant identification and accountability, agreement on a standard type of database and a standard type of format, standardization of types of information included in the database, standardization of data entry and retrieval, standardization of search criteria, standardization of computer hardware and software and web access capability. Legal considerations include patient confidentiality in compliance with all HIPPA regulations and register security. Fortunately, we now live in the computer age where people are very familiar with computer databases and search engines such as Google to obtain information on their own personal computers and the public is also very aware of password and encrypted security measures to protect individual confidentiality and rights. *Example of the Ortho-tag Total Knee and Total Hip Registry Radiofrequency Identification and Monitoring Technology: A Possible Solution We propose that the use of radiofrequency tags in conjunction with a biomedical reader will provide a noninvasive technology that is able to provide information about the state of the biological environment of the implant, manufacturing information about the implant, and surgical/arthroplasty information about the implant. Our plan represents an extension of the use of radiofrequency technology summarized in a recent report by Rand Europe, part of the Rand Corporation. The report, titled “Study on the requirements and options for RFID application in healthcare: Identifying areas for Radio Frequency Identification Deployment in Healthcare Delivery: A Review of Relevant Literature,” summarized results of a systematic review of peer reviewed and other literature dealing with radiofrequency identification (RFID) in health care (Vilamovska, et al 2009). Data abstracted from 325 items resulted in the development of four categories of RFID-enabling functions including tracking, identification and authentication, automatic data collection and transfer, and sensing. Among the use of RFID for sensing potential is as an alternative to dangerous or invasive imaging. These included diagnosis of critical intestinal patency, passive RFID tags to monitor the proper positioning of the endotracheal tube during intubation, and passive RFID tag use for patient comfort and cold sore prevention. We propose to extend the list to include the use of passive RFID tags in obtaining information about and monitoring the condition of hip and knee implants. As applied to our proposed use, the most practical solution is the combined use of radiofrequency tags and biometric readers. Our proposed application is to use RFID tags, in conjunction with a touch probe reader, to obtain information about three domains: (1) manufacturing information about the implant (e.g., model, manufacturer, manufacturing date, ID number); (2) information about the clinical aspects of the implant (e.g., date and time of implant, surgeon completing the implant); and (3) information about the biological conditions of the area surrounding the implant (e.g., initially we will use a temperature sensor; when available we will add a sensor for pH level, another bioindicator of infection). •Research already conducted at the University of Pittsburgh RFID Center of Excellence reveals that the transcutaneous energy/communication problem of metal hip and knee implants can be overcome by replacing the interrogator antenna with a touch probe consisting of two metallic electrodes (U. S. Patent No. 7,825,807, issued November 2, 2010) Health Relevance The development of a non-invasive means for monitoring the manufacturing and clinical characteristics of implants as well as the biological status of surrounding tissue has major implications for public health. This is particularly the case when, as estimated, within the next 20 years nearly 5 million hip and knee implants will be placed thus increasing the need for monitoring these prostheses. The use of RF technology is particularly important in addressing this need insofar as other current monitoring methods are invasive and can involve surgical removal of the prosthesis. Further, the RF tag is attached to the prosthesis and does not significantly change its configuration. As such, no changes in surgical procedures or in the implant itself are required. Further, since the RF tag is passive and does not serve as the source of energy for the signal, its presence does not introduce increased risk for toxicity to the patient. The RF tag and touch probe reader will allow physicians and manufacturers to: (a) insure that the device implanted is not counterfeit and has been adequately tested and approved by FDA; (b) not rely on written patient records to obtain information about the clinical/medical aspects of the implant procedure; and (c) monitor the biological environment of the implant in order to monitor for deep tissue infection without using invasive techniques We propose an alternative method for maintaining and accessing the technical characteristics of implanted medical devices by combining our patented technologies and expertise in the science of radiofrequency identification (RFID), bioengineering and Orthopaedic Surgery: Knowledge of the technical characteristics of implanted medical devices and surrounding tissue is very important to ensure patient safety and quality control. However, one of the major technical problems in accomplishing this is the inability to noninvasively obtain implant and surrounding environment information. To date, the only way to obtain medical implant information is from records that are not always available or through the use of invasive techniques. Our Ortho-tag technology permits information access in a rapid, noninvasive manner. The Ortho-tag system technology uses passive RFID devices to obtain information and monitor hip and knee implant condition. As applied, the most practical solution is the combined use of radiofrequency tags and biometric readers. This application will use RFID devices and a touch probe reader to obtain information about three domains: 1) Manufacturing information (model, manufacturer, manufacturing date, ID number) 2) Clinical aspects information (date and time of implant, surgeon completing the implant) 3) Biological conditions of the area surrounding the implant (temperature and pH sensor). Recent American Association of Orthopedic Surgeons practice guidelines for diagnosing deep periprosthetic joint infection, a major cause of implant revision, requires sampling blood and joint fluid and injecting radioisotopes into possibly infected joints. Assessment of implant wear, identification of age, type, and manufacturer for recall purposes, and counterfeit analysis can only be obtained from medical records that are not always available or by removing the implant. The Ortho-tag technology utilizes radiofrequency devices in conjunction with a biomedical reader providing a non-invasive technology that supplies implant information regarding the biological environment, manufacturing, and surgical/arthroplasty information. This significant application of tagging orthopedic implants makes the accompanying implant information available to orthopedic surgeons around the world no matter where the patient travels; however, it is one with potential challenges. First, the tag will be attached to a metallic implant - the worst media to allow passive reading. Second, reading the device through human tissue known to absorb RF energy makes energy delivered to the tag and backscattered response problematic. Both issues have successfully been addressed, and our research at the RFID Center of Excellence at the University of Pittsburgh has demonstrated: 1) RFID tags mounted on metallic orthopedic implants can be read 2) The use of volume conduction to read a passive RFID tag through saline (a surrogate for human tissue) 3) Harvesting of RF energy and communication through human tissue 4) The functionality of the touch probe to work directly on passive RFID tags by physically touching in the proximity of the tag without over-the-air RF transmission 5) Impedance match an RFID tag forming what is termed here as the ortho-tag. Working together we have demonstrated in the lab a very good working model of the Ortho-tag system and have proven scientifically RFID technology can be used to interact with orthopaedic implants in the body. With our Ortho-tag system we have overcome the barriers and difficulties of transmission of radiowaves through tissue and the problem of radiowave interference by metal implants. Utilizing the touch probe to power the RFID tag on the implanted hip or knee prosthesis reduces the amount of radiofrequency compared to over the air transmission, focuses the RF directly toward the tag, improves transmission of data and improves security of the information since the probe has to directly touch the patient’s skin for transcutaneuos transmission of the signal to the tag. Implementation of our Ortho-tag device on currently manufactured orthopaedic implants is an easy process that will not be costly to manufacturers with no design changes to the device as the ortho-tag is attached to a non-articular area on the prosthesis and covered with a polymer biocompatible seal. Biosensors can also be incorporated into the system to monitor the tissue environment around the implant. There is much competition between orthopaedic implant manufacturers and the first to offer a “smart implant” would have a significant advantage over others. This will encourage the orthopaedic and manufacturing communities to work together to use the vital information that can be obtained from implanted total joints to improve healthcare. In summary, we have invented and developed new technology that offers orthopaedic manufacturers, surgeons, hospitals and patients the opportunity to have “smart interactive orthopaedic implants” that will provide the user of our Ortho-tag system with vital data to enhance patient care, reduce cost and improve the quality of healthcare. This information can be incorporated in the future into a universal central data management computer and web based National Joint Registry. References: American Academy of Orthopedic Surgeons. Guideline on the Diagnosis of Periprosthetic Joint Infections of the Hip and Knee, 2010: http://www.aaos.org/Research/guidelines/PJIguideline.asp. Bozic, KJ, Ries, MD. The impact of infection after total hip arthroplasty on hospital and surgeon resource utilization. J Bone Joint Surg Am. 2005;87:1746-51. Integrated Healthcare Association. Orthopedics Data Compendium: Use, cost, and market structure for total joint replacement, 2006; http://www.iha.org/medical_device_od.html. Kurtz, S, Ong, K, Lau, E, Mowat, F, Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007; 89:780-785. National Center for Health Statistics, National Hospital Discharge Survey: 2005 Annual Summary with Detailed Diagnosis and Procedure Data. November 2002, http://www.cdc.gov/nchs/about/major/hdasd/listpubs.htm/. Parvizi, J. New CPG on diagnosing periprosthetic infections. American Academy of Orthopedic Surgeons. 2010: http://www.aaos.org/news/aaosnow/aug10/cover1.asp. Poultsides, LA, Liaopoulos, LL, Malizos, KN. The orthopaedic forum: The Socioeconomic impact of musculoskeletal infections. J Bone Joint Surg Am. 2010;92A:e13(1-12). Vilamovska, AM, Hatziandreu, E, Schindler, HR, Oranje-Nassau, C, deVries, H, Krapels, J. Study on the requirements and options for RFID application in healthcare: Identifying areas for Radio Frequency Identification deployment: A review of relevant literature. Rand Europe Technical Report, 2009: 1-110. Wilson, NA, Schneller, ES, Montgomery, K, Bozic, KJ. Hip and knee implants: Current trends and policy considerations. Health Affairs. 2008; 27:1587-1598. Röder C, El-Kerdi A Centralized Total Joint Replacement Registry Using Web-Based Technologies. JBJS Volume 86-A Number 9, September 2004 Maloney WJ. National joint replacement registries: has the time come? J Bone Joint Surg Am. 2001;83:1582-5. Herberts P, Malchau H. Long-term registration has improved the quality of hip replacement: a review of the Swedish THR Register comparing160,000 cases. Acta Orthop Scand. 2000;71:111-21. Paterson D. The International Documentation and Evaluation System (IDES). Orthopedics. 1993;16:11-4. Röder C, Eggli S, EL-Kerdi A, Müller U, Am-brose T, Röösli E, Busato A, Aebi M. The International Documentation and Evaluation System (IDES)—10-years experience. Int Orthop. 2003; 27:259-61. Röder C, Parvizi J, Eggli S, Berry DJ, Müller ME, Busato A. Demographic factors affecting long-term outcome of total hip arthroplasty. Clin Orthop. 2003;417:62-73. Röder C, Eggli S, Aebi M, Busato A. The validity of clinical examination in the diagnosis of loosening of components in total hip arthroplasty. J Bone Joint Surg Br. 2003;85:37-44. Müller U, Gautier E, Roeder C, Busato A. The relationship between cup design and the radiological signs of aseptic loosening in total hip arthroplasty. J Bone Joint Surg Br. 2003;85:31-6. Patents Cited U.S. Patent 7,333,013 “Medical Implant Device with RFID Tag and Method of Identification”; J. Lee Berger US Patent #7,333,013 “RF tag containing biological sensors as well as manufacturing and clinical information is placed on the prosthesis prior to implantation”; Marlin H. Mickle, et al US Patent #7,825,807 “Transponder Networks and Transponder Systems Employing a Touch Probe Reader Device”; Marlin H. Mickle, et al U.S. Patent No. 6,847,844 Method of Data Communication with Implanted Device and Associated Apparatus, Mingui Sun, Robert Sclabassi, Marlin H. Mickle, U.S. Patent No. 7,228,183, June 5, 2007 Method of Data Communication with Implanted Device and Associated Apparatus, Mingui Sun, Robert Sclabassi, Marlin H. Mickle