MRI Questionaire
advertisement

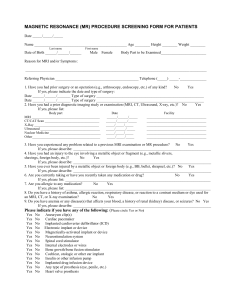
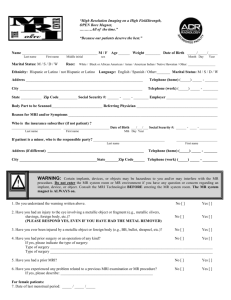
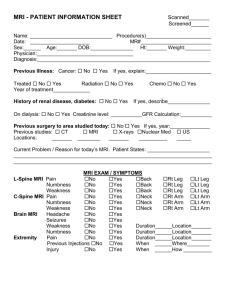
more than just x-rays MRI QUESTIONAIRE NAME (L, F):_______________________________ MR#_______________ REFERRING DR: _________________ CC: __________ WT: __________HT:_______ SEX: M __ F __ DOB: ___________ AGE: ______ IMAGES@TOS:_____________ EXAM TYPE: _____________________________________ PRIOR SURG TO REGION: YES NO REASON FOR EXAM/SYMPTOMS: ____________________________________________________________________________ Prior MRI of same area? Prior CT of same area? Prior XRay of same area? Ever diagnosed with Cancer? Previous Radiation Therapy? Previous Chemotherapy? Yes Yes Yes Yes Yes Yes ☐ No ☐ ☐ No ☐ ☐ No ☐ ☐ No ☐ ☐ No ☐ ☐ No ☐ Where: ____________________________________ Where: ____________________________________ Where: ____________________________________ Type: _____________________________________ When: ____________________________________ When: _____________________________________ Any history of kidney disease or renal failure? Yes ☐ No ☐ Is Patient Diabetic? Yes ☐ No ☐ Is Patient Hypertensive? Yes ☐ No ☐ Any Surg in past 8 weeks? Yes ☐ No ☐ Have you ever had head, neck, or brain surgery? Yes ☐ No ☐ Specify: _______________________________________________________________________________________ Are you pregnant? Yes ☐ No ☐ Are you Breastfeeding? Yes ☐ No ☐ Are you Claustrophobic? Yes ☐ No ☐ Have you ever had an injury to your eyes involving metallic slivers or shavings? Yes ☐ No ☐ Please indicate if you have any of the following: Cardiac Pacemaker Heart Valve Prosthesis Aneurysm Clip Eye Implant Implanted Defibrillator Implanted Drug Infusion Device Implanted Electrical or Mechanical Device Hearing Aid Cochlear Implant Joint Replacement Removable Bridgework or Dentures Swan-Ganz Catheter Vascular Stents or Filters: Yes ☐ No Yes ☐ No Yes ☐ No Yes ☐ No Yes ☐ No Yes ☐ No Yes ☐ No Yes ☐ No Yes ☐ No Yes ☐ No Yes ☐ No Yes ☐ No Yes ☐ No ☐ (INFORM STAFF NOW) ☐ ☐ ☐ ☐ ☐ ☐ Type: __________________________ ☐ (REMOVE BEFORE ENTERING MR ROOM) ☐ ☐ TYPE: _________ WHEN: ______________ ☐ ☐ ☐ TYPE: __________WHEN:_____________ I CERTIFY THAT I HAVE DOUBLE CHECKED MY POCKETS AND HAVE LEFT ALL PERSONAL ITEMS IN THE LOCKER. SMDI IS NOT RESPONSIBLE FOR ANY ITEMS LEFT ON MY PERSON. I CERTIFY THAT ALL THE INFORMATION LISTED ABOVE IS CORRECT AND TRUE TO THE BEST OF MY KNOWLEDGE. I CONSENT TO THE ADMINISTRATION OF THE ABOVE DIAGNOSTIC TEST(S). Patient Signature: ___________________________________________Date:_______________ Tech/Comments: _____________________________________________ Date:________ Magnevist cc:__________ Inj Site:_______ www.smdi.net 8303 S. Suncoast Blvd • Homosassa, FL 34446 Phone (352)628-9900 • Fax (352)628-9700