physics and clinical measurement for the primary frca
advertisement

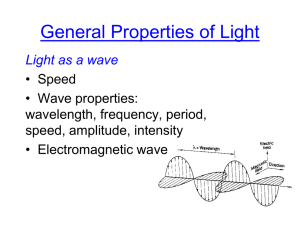
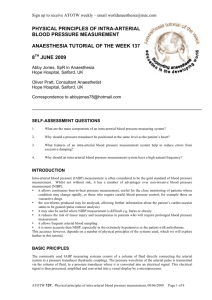
PHYSICS AND CLINICAL MEASUREMENT FOR THE PRIMARY FRCA Ian Wrench - 2002: Blood pressure measurement Lasers Measurement of pH/ pCO2/ O2 Physics of gases Source material: Basic physics and measurement in anaesthesia - Davis, Parbrook and Kenny, fourth edition, Butterworth and Heineman. Principles of Clinical Measurement. MK Sykes, MD Vickers, CJ Hull. Second Edition. Blackwell Scientific Publications. International Practice of Anaesthesia. C Prys-Roberts, BR Brown Jr. First Edition. Butterworth Heinemann. Understanding Anaesthesia Equipment, JA Dorsch, SE Dorsch. Fourth Edition. William and Wilkins. Ward’s Anaesthetic Equipment. A Davey, JTB Moyle, CS Ward. Third Edition. Saunders. 1 DIRECT BLOOD PRESSURE MEASUREMENT (Definition of Pressure = Force over unit area) Parts of a system for invasive blood pressure measurement: Heparinised saline under pressure Monitor Fluid filled tubing Amplifier Transducer Wire for electrical signal 3 way tap Constriction + flushing device Cannula Figure 1 Components of an intra-arterial pressure measurement system The cannula is usually sited in a large peripheral artery such as the radial artery. The cannula is kept free of clot by a continuous flushing system. A bag of heparinised normal saline is connected to the cannula by rigid walled plastic tubing. The bag is pressurised up to 300 mm Hg to prevent reflux of intra-arterial blood into the tubing. Integral to the system is a flushing device where there is a constriction to flow. Relief of the constriction causes flushing of the cannula under high pressure. Whilst the constriction is in place the cannula is flushed slowly at 3 to 4 ml/ hour. In order for the arterial pressure waveform to be represented electronically it must be changed into an electrical signal by means of a pressure transducer. A transducer is a device that converts one form of energy into another. In the case of an arterial line this change occurs by means of a resistance which varies according to the strain which is put on it by the changing blood pressure. The resistance is part of a Wheatstone bridge (figure 2). In a Wheatstone bridge a battery acts as a current source across 4 resistances (R). A galvanometer is attached at the junctions of R1-R2 and R3-R4. If 2 the equation R1/R2 = R3/R4 is true then there is no flow of current and therefore no deflection on the galvanometer. R1 R2 Galvanometer R3 R4 Figure 2: A Wheatstone bridge In a pressure transducer (figure 3) as the pressure increases so the diaphragm is moved to the right shortening the strain gauge and changing the resistance R4 which is part of a Wheatstone bridge as above. As the resistance R4 changes, so the equation R1/R2 = R3/R4 is no longer true and current flows across the galvanometer. The amount of current flowing is then equated with the pressure and thus a value derived. Saline under Pressure Strain gauge R4 Diaphragm Figure 3: A pressure transducer. More sophisticated transducers are set up so that all 4 resistances are incorporated as strain guages. The resistances are set up in such a way that 2 of them on opposite sides of the bridge increase and the other 2 decrease. This has the effect of magnifying any change that occurs. Fourier analysis Fourier was a 19th century French mathematician who showed that even complex repetitive waveforms could be analysed as being the sum of a series of much simpler waveforms called sinusoids (Figure 4). A complex waveform contains a fundamental 3 frequency that is the lowest frequency also known as the first harmonic. For arterial blood pressure this equates to the heart rate. There are then a series of harmonics that are in phase with the fundamental frequency i.e. in the same direction and passing through zero amplitude together. The second harmonic is a sinusoidal waveform that has twice the frequency and the third harmonic 3 times the frequency of the first harmonic and so on. A complex waveform such as arterial pressure may have as many as 30 harmonics, however the lower harmonics have the greatest amplitude (peak to trough height) and contribute most to the final waveform. Because of this reproducing the fundamental and the first 10 harmonics can often obtain a rough approximation of the arterial pressure waveform. If the heart rate is 60 beats per minute then this equals one cycle per second (1 Hz) so that the fundamental frequency is 1 Hz. The first 10 harmonics for this waveform would go up to 10 Hz so that any recording system would require a frequency response that was undistorted up to 10 Hz to accurately reproduce the original. If the heart rate were 120 then the frequency response would need to be 20 Hz. It has been shown that most of the important information of pressure waveforms from the heart and great vessels is contained in the range 0 – 20Hz. A properly designed measurement system should therefore produce minimal amplitude and phase distortion for this range of frequencies. Waveform First harmonic (fundamental) Second harmonic Amplitude of waveform The harmonics are in phase i.e. in the same direction and passing through zero amplitude together. Figure 4 Fourier analysis of a simple waveform showing the first (fundamental) and second harmonics. The first harmonic equates to the heart rate for blood pressure. The harmonics are in phase i.e. in the same direction and passing through zero amplitude together. The first harmonic has the greatest amplitude (peak to trough height) and contributes most to the final waveform. Sources of error – resonant frequency and damping Most cannula-tap-tube-tap-transducer combinations used for invasive monitoring are so called second order systems that tend to oscillate after being displaced. The characteristics of a second order system producing inaccuracies are related to its 4 natural or resonant frequency (the frequency at which it oscillates freely) and the damping coefficient which is an index of the tendency of the system to prevent or minimise these oscillations. As the frequency of the BP waveform approaches the natural frequency of the system, oscillations of the system augment the recorded values, leading to exaggerated pulse pressures (Figure 5). Any damping present in the system will compensate for this effect, however over-damping will result in a blunted trace and underestimation of the pulse pressure (Figure 5). Errors in the amplitude of the recorded waveform will be minimal if the resonant frequency of the system is well above the significant harmonics of the waveform being measured. In practice this is difficult to achieve. To maximise the natural frequency, a system should incorporate a short, wide stiff cannula connected to a transducer with a stiff low-displacement diaphragm. A large fluid mass, elastic tubing, long connectors, excessive connections and air bubbles all tend to reduce the natural frequency and increase the damping coefficient of the system. In practice a 4 cm 20 gauge non-tapered arterial cannula connected to a lowdisplacement pressure transducer by non-compliant plastic tubing and a single 3 way stopcock should have an adequate amplitude/ frequency response up to 25Hz. Whilst such a system may have a natural frequency which is close to the significant harmonics of the measured waveform, this is compensated for by optimal damping. Optimal damping represents the best compromise between the speed of response of the system and accuracy of registration of amplitude. 150 m m H g 100 50 (a (b (c Figure 5: Three examples of frequency response in a catheter transducer system – a) the waveform is correctly reproduced with optimal damping and an appropriate frequency response, b) an underdamped system with a low frequency response resulting in exaggeration of high frequencies so that systolic pressure is overestimated and diastolic pressure underestimated, c) an overdamped system due to an air bubble or a kinked catheter so that systolic pressure is underestimated and diastolic pressure overestimated. In all 3 cases the mean pressure is the same. 5 Calibration of an arterial line It is the case that for most medical equipment, three-point calibration is required. The zero point is when the system is open to air and two other points are taken by attaching a mercury manometer to the measuring system and using a point in the working range (e.g. 100 mmHg) and another in the high range (200 mmHg): 200 = high range Arterial line 100 = working range 0 = Zero Mercury manometer INDIRECT BLOOD PRESSURE MEASUREMENT Mercury manometer The cuff is centred over the brachial artery The cuff is 20% wider than the diameter of the arm The mercury column must be vertical The mercury column is not under a vacuum but vents to air. Air vent Mercury Cuff Automatic blood pressure measurement The cuff is inflated to above systolic pressure The cuff is slowly deflated Systolic BP = onset of pulsations Mean BP = point of maximum oscillation (most accurately measured) Diastolic BP is derived 6 LASERS The term laser stands for Light Amplification by Stimulated Emission of Radiation. The stimulated laser medium gives off energy in the form of light which is then amplified and emitted as the laser beam. The laser beam may deliver large amounts of energy to a very small area with great accuracy for example for cutting or coagulation. The light is a non-divergent pencil which is coherent (all waves are in phase in time and space) polarised and monochromatic (all the same wavelength). The laser medium gives the name of the laser. The medium may be solid (Nd Yag), liquid or gas (CO2, Argon) and determines the wavelength of the emitted radiation. The laser medium is contained within the optical cavity that contains mirrors to reflect and increase the energy of the stimulated emission. One of the mirrors is not 100% reflective and therefore allows the laser beam to escape. Energy is supplied to the laser medium by the pumping source that is a xenon flash lamp for a solid medium and an electric discharge for a gaseous medium. When an atom (it may also be a molecule or ion depending on the medium) of the medium in the ground state absorbs a photon of energy from the pumping source, the atom becomes excited. The excited atom then emits a photon of energy as it falls back to its ground state. If the atom absorbs another photon of energy whilst in the excited state, it emits 2 photons of energy as it falls back to the ground state and this is known as stimulated emission. The emitted radiation then causes further atoms to become excited and further photons of light to be released. Thus a chain reaction occurs producing an intense source of light energy which escapes through the area of the mirror which is only partly reflecting. Mirror Laser medium Partly reflecting mirror Laser Beam Pumping source Figure 6 – Diagram to show the working principle of a laser. There are 3 types of laser in common clinical use. The CO2 laser emits light of a wavelength of 10,600 nm which is strongly absorbed by tissues and enables precise surgical cutting with coagulation and sealing at the same time. The CO2 laser is most often used for laser to the larynx. The neodymium, yttrium, aluminium, garnet (Nd Yag) laser has a solid medium which emits light of the wavelength 1060 nm. This may be transmitted down 7 fibreoptics to be absorbed by darkly pigmented tissues. It may be used for photocoagulation of gastrointestinal bleeding lesions and bronchial carcinomas. The wavelength of Argon lasers is 500 nm and they are used for port wine stains and retinal work. 8 Measurement of pH/ pCO2/ O2 (blood gases) Introduction Measurement of all of the above depends on the alteration of the flow of electricity in relation to the concentration of the substance to be measured. A heparinised arterial blood sample is taken anaerobically. If necessary, the sample is stored in ice to prevent metabolism prior to being injected into the blood gas machine. The blood within the machine is kept at 370C. The blood is separated from the electrodes by a plastic membrane to prevent the accumulation of blood proteins on the electrodes. The substance to be measured diffuses across the plastic membrane to reach the electrodes and influence the flow of electricity. The measurement of O2 – Clark electrode: Anode = Ag/ AgCl Cathode = Platinum Anode and cathode are in electrolyte e.g. KCL Voltage of 0.6V applied between anode and cathode Reaction at anode – Ag (electrode) + Cl- (electrolyte) -> AgCl + electrons Reaction at cathode – O2 + 4e + H2O -> 4(OH)- (similar to Krebs cycle) METER Electrolyte Ag/ AgCl anode Platinum cathode Plastic membrane BLOOD 37oC How does the fuel cell differ from the Clark electrode? Fuel Cell: Used for O2 measurement in gas not liquid Anode = lead Cathode = gold mesh Electrolyte = KOH No voltage is applied as the fuel cell acts as a battery Reaction at anode – Pb + 2(OH)- ->PbO + H2O + 2e Reaction at cathode – same as Clark electrode 9 The measurement of H+: Meter Measuring electrode (Ag/ AgCl Reference electrode (Ag/ AgCl) Saturated KCl solution Buffer solution H+ sensitive glass Plastic membrane BLOOD 37oC The concentration of hydrogen ions within the measuring electrode is kept constant so that the flow of current is dependent upon the concentration of hydrogen ions within the blood. The measurement of CO2 – Severinghaus electrode: METER Bicarbonate Electrodes H+ sensitive glass covered by nylon mesh Plastic membrane BLOOD 37oC Carbon dioxide reacts with water to produce carbonic acid which dissociates to bicarbonate and hydrogen ions. Thus the H+ concentration is directly related to the CO2 concentration. 10 PHYSICS OF GASES Before considering the physics of gases it is necessary to start with the system upon which all our measurements are base the Systeme International d’unites (SI units). There are 7 basic SI units: 1 - Length = metre 2 - Mass = kilogram 3 - Time = seconds 4 - Current = ampere 5 - Temperature = Kelvin 6 - Luminous intensity = candela 7 - Amount of substance = mole All the other units are derived from the above 7, for example - Temperature in degree Celsius, force in Newtons, pressure in Pascals, energy in Joule or electron-volt, power in Watt, frequency in Hertz, and volume in cubic metres or Litres PHYSICS OF GASES 1) Some Definitions i) Pressure (= force per unit area) SI Unit = Pascal derived from Newton / metre sq. 1 atmosphere = 101.325 kilopascals = 1000 cm H2O = 15 LB sq. in Absolute Pressure = Pressure compared to a Vacuum Relative or Gauge Pressure = Pressure relative to atmospheric e.g. a full O2 Cylinder has an absolute pressure of 138 atmospheres but a relative pressure of 137 atmospheres. ii) Avogadro’s hypothesis = Equal volumes of gases at the same temperature and pressure contain equal number’s of molecules. Avogadro’s number = the number of molecules in a mole of substance = 6.02 x 1023 = 22.4 litres at standard temperature and pressure. iii) Critical temperature = the temperature above which a substance cannot be liquefied no matter how high the pressure. iv) Critical pressure = the vapour pressure of a substance at its critical temperature. v) Viscosity = a measure of the frictional forces between layers of the “liquid” as it flows along a tube. Units = pascal seconds. vi) Density = mass per unit volume. Units = kgm-3 11 2) Gas Laws (all for a given mass of gas – see also figure 7). i) Boyle’s law - at constant temperature volume is inversely proportional to pressure:PV = k1 ii) Charles’ law - at constant pressure temperature is directly proportional to volume:V = k2T iii) Third gas law = at constant volume pressure is directly proportional to temperature:P = k3 T The universal gas constant - PV = constant T Clinical application of gas laws - The pressure in an oxygen cylinder declines linearly as it empties (Boyle’s law) provided the temperature remains constant. In practice as the gas remaining in the cylinder expands adiabatically (without heat exchange with its surroundings) it cools and therefore the process is non- linear. 3) Gas Flow (see figure 8) i) Laminar flow - the fluid moves with no eddies or currents, usually at low flow rates in smooth tubes. The flow in the centre is greatest with that near the wall approaching zero. Flow is calculated by the Hagen-Poiseuille formula = Pr4 8l P = pressure, r = radius of the tube, Q = flow, l = length, = viscosity of the fluid. Q ii) Turbulent flow - the flow is not ordered, there are eddies and currents. It occurs at high flow rates as predicted by a Reynolds number of greater than 2000:Reynolds’ number = r = viscosity, = linear velocity, = density, r = radius of the tube. Clinical relevance - the rotameter - at low flow rates the flow is laminar and therefore viscosity determines the bobbin position, at high rates the flow is turbulent and density determines the position. iii) The Bernoulli Principle - When there is flow in a tube the pressure is least at its narrowest point. The pressure may fall to below atmospheric at this point and may cause entrainment e.g. the venturri mask, nebulisers portable suction etc. 12 OTHER HEADINGS FOR PHYSICS AND CLINICAL MEASUREMENT Nerve stimulators Measurement of gas concentration Temperature and humidity Capnography Pulse oximetry Volume and flow in gases and liquids Pulmonary function tests Mathematical concepts - sinusoids, exponential functions, parabolas. Simple mechanics - mass, force, work and power. Heat - simple calorimetry, conduction, convection, radiation. Freezing point, melting point, latent heat, vapour pressure. 13