Supplementary Information (doc 1174K)
advertisement
")
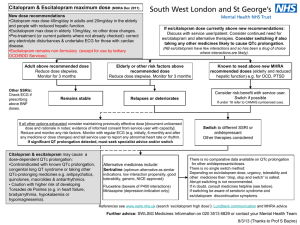
SUPPLEMENTARY INFORMATION Clinical methods and results at National Institutes of Mental Health, Bethesda Female and male subjects 18 to 65 years of age with MDD currently experiencing a major depressive episode without psychotic features lasting at least four weeks, a score of ≥ 20 MADRS, and no more than three failed antidepressant trials within the current major depressive episode were enrolled. Diagnoses were established by clinical evaluation and by using the Structured Clinical Interview for DSM-IV (SCID) (1). After consenting to the study, subjects underwent a physical exam, psychiatric and medical history, routine laboratory analyses, a pregnancy test, an electrocardiogram (ECG), the assessment of vital signs. Depression severity was assessed using the Montgomery–Åsberg Depression Rating Scale (MADRS) (2) and the Quick Inventory of Depressive Symptomatology-C16 (QIDS) (3). Subjects were excluded if they had any serious unstable medical disorders, such as uncontrolled diabetes, hypertension, or seizures. Other exclusion criteria included pregnancy or breastfeeding, history of substance abuse within the past three months or alcohol use within the past seven days, any history of psychotic disorder, bipolar disorder, or current active suicidal ideation. Subjects who had previously failed to respond to citalopram were excluded. Patients were not permitted to participate in psychotherapy for the duration of the study. All subjects provided written informed consent as approved by the National Institutes of Health (NIH) Combined Neuroscience Institutional Review Board. The first period of the study involved screening, taper from non-allowed medications, and a twoweek interval free of psychotropic medications (if patients had been taking such medications). Concomitant medications were not allowed and were tapered and discontinued over at least two weeks prior to study treatment. Citalopram treatment was initiated; doses were titrated based on the Measured Based Care Approach as used in the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study (4). The patients were initially put on 10 mg citalopram. The dosing of citalopram was then optimized on an individual basis and on a weekly basis to achieve optimal treatment response. At the end of the second week, when blood was drawn for p11 measurements, all but one included patient received 20 mg of citalopram. The dosing of citalopram continued to be optimized on a weekly basis. At the eigth week, when blood was drawn again, two patients received 1 20 mg, two patients 30 mg, five patients 40 mg, one patient 50 mg and three patients 60 mg. During the study, subjects were not permitted to receive additional medications or alcohol (a full list of non-allowed medication is available upon request). The major finding of this study is that early reduction in p11 levels in Natural Killer cells and monocytes predicts the likelihood of antidepressant response to chronic citalopram. The data has been analyzed with regards to possible confounding factors, including citalopram dose, baseline depression severity, age and gender. As described above, all but one patient received 20 mg of citalopram after two weeks of treatment and removal of this patient from the data analysis did not change the outcome of the study. The dosing of citalopram at the early timepoint when p11 was measured is not a confounding factor. The treatment of citalopram was then optimized on an individual basis and on a weekly basis to achieve optimal treatment response. There was no correlation between treatment response and citalopram dose. All but one patient had a MADRS score (20-34) corresponding to moderate depression at baseline. When the data were analyzed without the patient with severe depression (MADRS score 41), it was still significant. There were no correlations between age and p11 levels at any studied timepoint or between age and antidepressant response. When both genders combined (Fig 1), or only men , were analyzed, p11 was reduced in NK cells after two weeks of citalopram and this reduction correlated with clinical improvements on MADRS as assessed after eight weeks of citalopram. A similar non-significant trend was also found when only women were analyzed. With regards to p11 levels in monocytes, a significant correlation between reduced P11 after 2 weeks and clinical improvements on MADRS after eight weeks of citalopram, was found when both genders were combined (Fig 1). However, only non-significant trends were found when men or women were analyzed as separate groups. The later effects are most likely due to the low number of patients. 14 out of 26 patients had all three sets of blood collected. Baseline depression severity, gender or age were different between patients with complete and non complete blood draws. Treatment response seems however to partly differ between patients with non complete versus complete 2 blood draws. 10 of the 14 patients that had complete blood sample collections responded to the treatment, whereas four did not. In one non-responding patient, there was a technical problem with the p11 measurement in NK cells and T cells. Among the patients with non complete blood draws, five non-responding patients and five early responding patients dropped out of the study prematurely. Two responding patients failed to give blood samples on all occasions. Clinical methods and results of MDD patients recruited at UT Southwestern in Dallas A separate group of eleven patients with MDD in a current major depressive episode were recruited at UT Southwestern in Dallas along the inclusion and exclusion criteria listed above. Their average (SD) age was 39.7±8.9 and there were seven females and four males. At screening they were free of psychotropic medications for at least two weeks and completed a medical and psychiatric history; diagnosis was confirmed using the SCID (1). Patients were assessed using the Inventory of Depressive Symptomatology-C30 (IDS) (5) and treated with citalopram for twelve weeks. Three patients immediately dropped out of the study. The remaining eigth patients were initially put on 20 mg citalopram and at the end of the first week, when blood was drawn for p11 measurements, all patients received 20 mg of citalopram. The dosing of citalopram continued then to be optimized. At week twelve, when blood was drawn again,all subjects, but one, received 40 mg of citalopram. Fasting blood samples were drawn, and PBMCs were prepared at baseline and, for most patients, after one and twelve weeks of citalopram treatment. Eight patients completed the study, but two of these individuals did not leave blood at all occasions. All the patients with complete blood sample collections responded to the treatment. As stated in the main text, p11 levels in NK cells and monocytes after one week of citalopram treatment correlated with improvements in IDS ratings after twelve weeks of citalopram (Fig S3). The data have been analyzed with regards to possible confounding factors, including citalopram dose, baseline depression severity, age and gender. All patients in the UT Southwestern cohort received 20 mg of citalopram after one week when p11 measurements were made. All but one patient in the UT Southwestern cohort received 40 mg of citalopram after twelve weeks of treatment. Removal of the patient that had a persistent 3 antidepressant response at 20 mg of citalopram did not change the outcome of the data for p11 in NK cells, but led to a loss of the significant correlation between p11 and clinical response found in monocytes. This is likely due to the very very low number of patients. All the patients had moderate depression severity at baseline. There were no correlations between age and p11 levels at any studied timepoint or between age and antidepressant response. There were too few patients to examine effects of gender. Thus, data from this group replicated findings from the MDD patients recruited at the NIMH, indicating that early reductions of p11 levels in NK cells and monocytes can predict a persistent antidepressant response to citalopram. Different rating scales were used to examine depressive symptomatology in the two cohorts, but it should be noted that the 16 items in the QIDS are included among the 30 items of the IDS. Both the QIDS and the IDS have highly acceptable psychometric properties and are treatment sensitive measures of symptom severity in depression (6). Conflict of Interest Madhukar H. Trivedi is or has been an advisor/consultant to: Abbott Laboratories, Inc., Abdi Ibrahim, Akzo (Organon Pharmaceuticals Inc.), Alkermes, AstraZeneca, Axon Advisors, BristolMyers Squibb Company, Cephalon, Inc., Cerecor, Concert Pharmaceuticals, Inc., Eli Lilly & Company, Evotec, Fabre Kramer Pharmaceuticals, Inc., Forest Pharmaceuticals, GlaxoSmithKline, Janssen Global Services, LLC, Janssen Pharmaceutica Products, LP, Johnson & Johnson PRD, Libby, Lundbeck, Meade Johnson, MedAvante, Medtronic, Merck, Mitsubishi Tanabe Pharma Development America, Inc., Naurex, Neuronetics, Otsuka Pharmaceuticals, Pamlab, Parke-Davis Pharmaceuticals, Inc., Pfizer Inc., PgxHealth, Phoenix Marketing Solutions, Rexahn Pharmaceuticals, Ridge Diagnostics, Roche Products Ltd., Sepracor, SHIRE Development, Sierra, SK Life and Science, Sunovion, Takeda, Tal Medical/Puretech Venture, Targacept, Transcept, VantagePoint, Vivus, and Wyeth-Ayerst Laboratories. In addition, he has received research support from: Agency for Healthcare Research and Quality (AHRQ), Corcept Therapeutics, Inc., Cyberonics, Inc., National Alliance for Research in Schizophrenia and Depression, National Institute of Mental 4 Health, National Institute on Drug Abuse, Novartis, Pharmacia & Upjohn, Predix Pharmaceuticals (Epix), and Solvay Pharmaceuticals, Inc. REFERENCES 1. First, Michael B., Spitzer, Robert L, Gibbon Miriam, and Williams, Janet B.W.: Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition. (SCIDI/P) New York: Biometrics Research, New York State Psychiatric Institute, November 2002. 2. Montgomery SA, Asberg M Brit J Psychiatry 1979; 134: 382–389. 3. Rush AJ, Trivedi MH, Ibrahim HM, Carmody TJ, Arnow B, Klein DN et al. Biol Psychiatry 2003; 54: 573-583. 4. Rush AJ, Fava M, Wisniewski SR, Lavori PW, Trivedi MH, Sackeim HA et al. Control Clin Trials 2004; 25: 119-142. 5. Rush, A.J., Gullion, C.M., Basco, M.R., Jarrett, R.B. and Trivedi, M.H. Psychological Medicine 1996; 26: 477-486. 6. Trivedi MH, Rush AJ, Ibrahim HM, Carmody TJ, Biggs MM, Suppes T et al. Psychol Med 2004; 34: 73-82. 5 CD56 Side scatter NK cells T cells Forward scatter CD3 Forward scatter Figure S1. Forward scatter Side scatter Side scatter Side scatter monocytes CD3 CD56 CD14 Flow cytometry analysis of fluorescently labeled PBMCs. Representative flow cytometry analysis of PBMC stained with fluorescently labeled antibodies to CD3, CD56, and CD14. In the upper panels, NK cells and T cells were identified as CD3-CD56+ and CD3+ lymphocytes, respectively. In lower panels, monocytes were identified as CD3-CD56-CD14+ leukocytes. 6 A NK cells B Monocytes C T cells Figure S2. p11 in NK cells, monocytes, and T cells and its regulation by citalopram in depressed individuals (NIMH patient group).Graphs showing median fluorescence intensity of p11 (percentage of baseline values) in (A) NK cells, (B) monocytes, and (C) T cells after two weeks of citalopram treatment and correlations with improvements in total QIDS score after eight weeks of citalopram treatment. Dots represent individual patients. Statistical analyses used Pearson’s correlation test and determined 95% confidence intervals. Statistical significance was defined as P<0.05. 7 A NK cells B Monocytes C T cells Figure S3. p11 in NK cells, monocytes, and T cells and its regulation by citalopram in depressed individuals (UT Southwestern patient group). Graphs showing median fluorescence intensity of p11 (percentage of baseline values) in (A) NK cells, (B) monocytes and (C) T cells after one week of citalopram treatment and correlations to improvements in total IDS score after twelve weeks of citalopram. Dots represent individual patients. Statistical analyses used Pearson’s correlation test and determined 95% confidence intervals. Statistical significance was defined as P<0.05. 8 A D G NK cells B Monocytes Monocytes E C T Tcells cells F H I Figure S4. Baseline p11 levels in NK cells, monocytes, and T cells and their correlations to MADRS ratings at baseline and following citalopram treatment (NIMH patient group). Graphs showing median fluorescence intensity of baseline p11 levels in (A, D, G) NK cells, (B, E, H) monocytes and (C, F, I) T cells and their correlations to (A-C) baseline MADRS scores, improvements in MADRS scores after (D-F) two weeks or (G-I) eight weeks of citalopram treatment. Dots represent individual patients. Statistical analyses were carried out using Pearson’s correlation test. Statistical significance was defined as P<0.05. 9