Lessons Learned as a Malpractice Expert Witness Consultant

Lessons Learned as a Malpractice Expert Witness Consultant
Andrew B Mick, OD, FAAO
Associate Clinical Professor
UC Berkeley School of Optometry
UCSF Department of Ophthalmology
Know the dangers of not dilating and “pseudo-dilating:” Asymptomatic rhegmatogenous retinal detachment
I. Small subset (~5%) of rhegmatogenous retinal detachments are asymptomatic
and diagnosed during routine examination
II. Clinical signs
A. Average age at diagnosis in the 40s as opposed to later in life for
symptomatic detachments
B. Can occur in the teens and 20s
C. Most commonly seen in the inferior quadrant with break seen inferiorly
D. Commonly caused by atrophic holes within lattice degeneration
E. From 35-65% occur with refractive errors greater than 5 diopters of
myopia
F. Greater than 90% of detachments extend posterior to the equator at
diagnosis
G. Up to 50% of patients do not have posterior vitreous detachments
H. Often detachments have signs of chronicity: demarcation lines (~40%)
and macrocysts
I. Significant percentage of patients have peripheral retina pathology in
the fellow eye
III. Management
A. Byer studied ten retinal detachments associated with lattice
degeneration up to 23 years and found 80% did not progress
B. Justifications to proceed to surgery include symptoms, documented
progression and immediate threat of foveal involvement
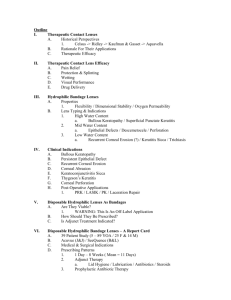
Small melanomas are clinically indistinguishable from choroidal nevi: Which to photograph and which to refer
I.
Choroidal nevi are incredibly common (5-8% of Caucasians) while choroidal melanoma is incredibly rare (six in every 1 million Caucasians)
II. Most authorities agree that documented growth over a relatively short period of time (1-2
years) is a convincing characteristic of mitotically active melanoma
III. Established risk factors for a small pigmented choroidal lesion being a melanoma
A.
Mnemonic: To Find Small Ocular Melanoma Using Helpful Hints Daily
B.
Thickness greater than 2 mm
C.
Presence of Subretinal fluid
D.
Overlying Orange pigment
E.
Margins near the optic disc
F.
Ultrasonographic Hollowness
G.
Absence of surrounding Halo
H.
Absence of overlying Drusen
IV. American Academy of Ophthalmology Preferred Practice Patterns
A.
“Patients with choroidal nevi who show no suspicious features require no treatment.
During the first year, they should be monitored twice; subsequently, they should be evaluated annually as long as the nevi remain stable.”
B.
“Patients who have one or two risk factors for malignant transformation should be monitored every four to six months.”
C.
“Patients with nevi and three or more suspicious features should be evaluated at an experienced center for management alternatives and possible treatment due to their increase risk of developing melanoma”
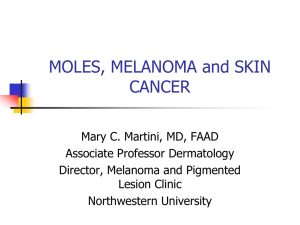
Know the laws and standards of care in the treatment of infectious keratitis: When should an ulcer be referred for cultures and sensitivities
I.
California State Law
A.
“If the patient has been diagnosed with a central corneal ulcer and the central ulcer has not improved 48 hours after the diagnosis, the optometrist shall refer the patient to an ophthalmologist”
II.
American Optometric Association Preferred Practice Patterns
A.
“Traditional management of corneal ulcers and severe infections begins with the acquisition of cultures on blood and chocolate agars, on heart and blood infusion (HBI, for fungi), or on thioglycolate medium or eugenic broth (for anaerobes), with gram-staining of smears for microscopic evaluation”
B.
“ Clinicians should recognize that the diagnosis and management of corneal infection continues to evolve. For example, community doctors tend to treat empirically, without initially collecting cultures and smears/staining, whereas such laboratory investigations prior to treatment remain the standard of care at hospitals and university medical centers.
In general, the trend toward treating peripheral and small, suspected corneal infections without laboratory investigation, while central and large corneal lesions are almost universally cultured prior to treatment.”
III.
American Academy of Ophthalmology Preferred Practice Patterns
A.
“The majority of community acquired cases of bacterial keratitis resolve with empiric therapy and are managed without smears and cultures. Smears and cultures are indicated however, in cases that involve a corneal infiltrate that is large and extends to the middle to deep stroma; that are chronic in nature or unresponsive to broad spectrum antibiotic therapy; or that have atypical clinical features suggestive of fungal, amoebic, or mycobacterial keratitis. Smears and cultures are often helpful in eyes that have unusual history, e.g., if there has been trauma with vegetable matter or if the patient wore contact lenses in a hot tub”
Not all acute optic neuropathies are non-arteritic anterior ischemic optic neuropathy
I.
There are very few optic neuropathies that do not require extensive work-ups
II.
(Glaucoma and non-arteritic AION are two common neuropathies requiring no or minimal work-up)
To diagnose non-arteritic AION without further work-up, should be CLASSIC case!
III. Classic clinical characteristics of non-arteritic AION
A.
Age greater than 60
B.
Presence of vascular risk factors (hypertension and diabetes)
C.
Vision loss noted within 2 hours of awakening
D.
Altitudinal visual field loss
E.
Disc at risk in fellow eye
F.
No progression beyond first 1-2 weeks
G.
No systemic symptoms of giant cell arteritis (Unexplained weight loss, neck or temporal pain, jaw claudication, general flu-like symptoms)
H.
ISOLATED!!! (No other neurologic signs/symptoms)
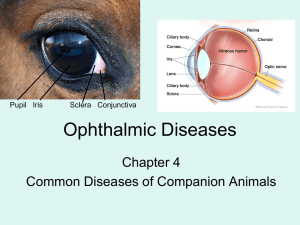
Not all ocular and adnexal infections are caused by Staph, Strep and Pseudomonas:
Community-associated methicillin resistant staphylococcus aureus (CA-MRSA)
I. MRSA initially described in 1960s as a healthcare associated infection (HA-
MRSA)
II. Defined risk factors for HA-MRSA
A. Hospitalization, surgery or dialysis within one year
B. Residence in a long-term care facility
C. Presence of permanent indwelling catheter or percutaneous device
III. Emerged as a more widespread cause of infection in community associated
infection in late 1990s (CA-MRSA)
IV. Since 1990s, rates of CA-MRSA have steadily increased
A. Using a national database, the percentage of CA-MRSA increased from
33% to 53% of all staph aureus isolates
B. CA-MRSA accounted for 59% of all soft tissue infections at a sample of
12 US emergency rooms in 2008
V. Defined risk factors for CA-MRSA:
A. Crowding (military recruits, prison inmates, childcare attendees, team-
sport participants, greater number of family members per bedroom)
B. Tattoo recipients
C. Ethnic minorities
D. Lower socioeconomic groups
E. Poor hygiene
F. Antibiotic therapy within six months
G. Abscess formation within soft tissue infection
VI. Ocular infections caused by CA-MRSA
A. Soft tissue infections most common (Internal hordeolum, preseptal
cellulitis, orbital cellulitis)
B. Blepharitis
C. Conjunctivitis
D. Keratitis
E. Endophthalmitis
VII. Treatment Recommendations
A. Avoid penicillin, fluoroquinolone and macrolid antibiotics
B. Oral doxycycline or bactrim (sulfamethoxazole and trimethoprim) for
soft tissue infections
C. Polymyxin B / trimethoprim solution and polymyxin B / bacitracin ung for
blepharitis, conjunctivitis and keratitis
D. Culture with lack of treatment response and increasing risk factors
E. Drain abscess if present in soft tissue infections
When prescribing orals compared to topicals you are greatly increasing possible liability:
Antibiotic therapy in anticoagulated patients
I. How antibiotics can disrupt anticoagulation
A. Antibiotics disrupt enteric flora that synthesize vitamin K
B. Vitamin K-dependent cofactors are greatly reduced, resulting in over-anticoagulation
C. Antibiotics can inhibit cytochrome p450 isozymes
D. Inhibition of isozymes responsible for the metabolism of warfarin, lead to
supratherapeutic plasma concentrations
II. Moderate risk of elevating INR in anticoagulated patients
A.
Amoxicillin
B.
Cephalexin
C.
Doxycycline
II. High risk of elevating INR in anticoagulated patients
A.
Fluoroquinolones
B.
Sulfonamides
C.
Macrolids
III. Management of patients requiring oral antibiotics who are anticoagulated
A.
The lowest possible risk antibiotic should be selected
B.
The lowest possible dose should be prescribed
C.
INR should be monitored closely while under therapy