Administrative Office St. Joseph`s Hospital Site, L301
advertisement

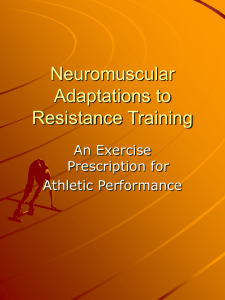
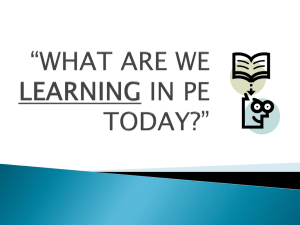
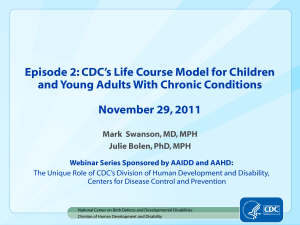
Administrative Office St. Joseph's Hospital Site, L301-10 50 Charlton Avenue East HAMILTON, Ontario, CANADA L8N 4A6 PHONE: (905) 521-6141 FAX: (905) 521-6142 http://www.fhs.mcmaster.ca/hrlmp/ Issue No. 67 QUARTERLY NEWSLETTER February 2003 Muscular Dystrophies, Recent Advances and the Use of Immunohistochemistry in Diagnosis Background The muscular dystrophies represent a large diverse group of inherited muscle diseases characterized generally by slowly progressive muscle weakness and atrophy. In these muscle disorders, the underlying defect is felt to be intrinsic to the skeletal muscle fibres. Duchenne’s muscular dystrophy was the first to be characterized. Most cases have an early childhood onset and are phenotypically severe. The responsible gene was isolated, cloned and localized to chromosome XP21, and the gene protein subsequently characterized (dystrophin). This protein was shown to be a sarcolemmal protein in the muscle fibres and by immunohistochemistry, was shown to be absent in the more severe cases (Duchenne’s form), and reduced in the less severe phenotypic form (Becker’s muscular dystrophy). From the clinical point of review, there remained a large group of milder, later onset muscle dystrophy diseases in which the underlying gene and protein abnormalities were unknown. However, during the last 10 years, as a consequence of the genetic revolution, a number of underlying responsible genes and muscle proteins have been identified in which defects underlie specific subtypes of this large group of muscular dystrophies clinically referred to as limb girdle muscular dystrophies (see table 1). As a result, recently, the application of routine immunohistochemistry to skeletal muscle biopsy specimens is allowing the specific subtyping of some of these forms of limb girdle muscular dystrophy. The Hamilton Regional Laboratory Medicine Program, through the Pathology/Neuropathology Department, receives a large number of muscle biopsies per annum (greater than 150), making it one of the larger neuromuscular referral pathology centers in North America. There is a strong clinical need then to characterize as accurately as possible from the pathologic point of view, the dystrophy sub-type of these cases. Recent Advances in Sub-classification of Limb Girdle Muscular Dystrophy Clinically defined limb girdle muscular dystrophy has been shown to be genetically quite heterogeneous, currently more than 10 different underlying genetic defects have been described, resulting in both autosomal dominant and recessive forms of muscle disease. A number of these genes have had their proteins isolated and characterized (see table 1). Many of these proteins are muscle fibre membrane proteins and their absence or significant reduction can be defined by routine immunohistochemistry from frozen skeletal muscle biopsy tissue (i.e. laminin alpha 2, dysferlin, sarcoglycan complexes) (see Fig. 1). Those proteins which are located in the muscle fibre sarcolemma would lead to an absent membrane staining pattern as a diagnostic abnormality. This is analogous to the earlier genetic and immunohistochemical work showing deficient membrane staining for dystrophin in Duchenne’s muscular dystrophy. Technically, this requires careful immunohistochemical characterization of the normal muscle fibre membrane staining pattern for these proteins. In addition, when test immunohistochemistry is being performed, staining for spectrin is performed, as an integral membrane protein. This serves as a useful control so that negative staining for the particular test protein, i.e. dysferlin, can be considered to be a specific protein deficiency if spectrin remains positive, so that it does not simply reflect generalized damage or loss of membrane proteins (see figure 2a and 2b). This immunohistochemical analysis potentially allows a rapid and routine diagnostic approach to be utilized on the biopsy tissue already available for the general pathology work-up. Current Applications In addition to dystrophin immunohistochemistry, used to diagnose Duchenne’s and Becker’s forms of muscular dystrophy, the Pathology/Immunohistochemistry laboratory can currently diagnose protein deficiencies of dysferlin, the sarcoglycan complex (gamma, alpha, beta and delta) laminin alpha 2 (Merosin), while caveolin-3 and calpain-3 are currently in a state of work in progress. This allows the potential specific diagnosis of six additional forms of limb girdle muscular dystrophy/distal muscular dystrophy, which would otherwise be considered part of the larger rubric of non-specific limb girdle muscular dystrophies. These are largely autosomal recessive muscle diseases with varying clinical courses and phenotypes (limb girdle muscular dystrophy type 2B, 2C, 2D, 2E and 2F, as well as the distal muscle dystrophy disease Miyoshi myopathy and congenital muscular dystrophy). Although presently specific therapies do not exist for these muscle diseases, delineating the specific form present, is clinically useful in predicting the subsequent behaviour and phenotype as well as for familial and genetic counseling. Furthermore, as the normal protein function of these molecules becomes better understood, specific therapeutic interventions may become apparent in the future. Figure 2a and 2b Figure 1 Legend Schematic characterization of the molecular organization of the integral membrane and associated proteins involved in skeletal muscle fibres in muscular dystrophies. Muscle biopsy from a limb girdle muscle dystrophy patient showing maintained sarcolemmal staining for spectrin with absent sarcolemmal membrane staining for dysferlin, diagnostic of limb girdle muscular dystrophe type 2B. Table 1 Protein Immunohistochemistry Dystrophy Diagnosis Pattern Dystrophin Membrane, absent Duchenne’s Dystrophin Membrane, reduced Becker’s Emerin Nuclear, absent Emery-Dreifuss Merosin (alpha-2 Membrane, absent Classic form, congenital muscular dystrophy Membrane, absent Limb girdle muscular dystrophy type 2B (Miyoshi laminin) Dysferlin myopathy) Gamma sarcoglycan Membrane, absent Limb girdle muscular dystrophy type 2C Alpha Membrane, absent Limb girdle muscular dystrophy type 2D Beta sarcoglycan Membrane, absent Limb girdle muscular dystrophy type 2E Delta Membrane, absent Limb girdle muscular dystrophy type 2F Caveolin-3 Membrane, absent Limb girdle muscular dystrophy type 1C Calpain-3 Cytoplasmic, absent Limb girdle muscular dystrophy type 2A sarcoglycan sarcoglycan Table 1 Legend: A partial listing of the proteins and correlated immunohistochemical staining pattern, used in the diagnosis of some of the major forms of muscular dystrophies. References 1. Cohn RD et al. Molecular basis of muscular dystrophies. Muscle & Nerve 2000;23:1456-1471. 2. Anderson LV et al. Characterization of monoclonal antibodies to calpain 3 and protein expression in muscle from patients with limb-girdle muscular dystrophy type 2A. Am J Pathol 1998;153:1169-1179. 3. Lim LE et al. The sarcoglycan complex in limb-girdle muscular dystrophy. Curr Opin Neurol 1998;11:443-452. 4. Matsuda C et al. Dysferlin is a surface membrane-associated protein that is absent in Miyoshi myopathy. Neurology 1999;53:1119-1122. 5. McNally EM et al. Caveolin-3 in muscular dystrophy. Hum Mol Genet 1998;7:871-877. Dr. J. Provias Discipline of Anatomic Pathology Hamilton Regional Laboratory Medicine Program Hamilton General Hospital Site