ASIAN ASSOCIATION OF PEDIATRIC SURGEONS
advertisement

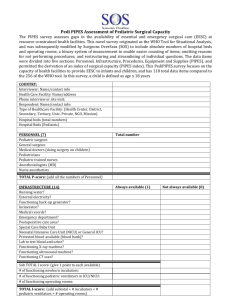
P1 AAPS ASIAN ASSOCIATION OF PEDIATRIC SURGEONS APPLICATION I. FORM FOR MEMBERSHIP GENERAL INFORMATION Name (Last) Country Citizenship Date of Birth [ ] Home Address Phone Phone preferable address Year of Graduation SURGICAL RESIDENCY Hospital IV. Location PEDIATRIC BOARDS, Dates SURGICAL RESIDENCY Hospital V. for mailing EDUCATION Medical School III. (Middle) [ ] Office Address [ ] Please check the II. (First) Location DEGREES, Dates TITLES, FELLOWSHIPS, HONOURS: Date VI. CATEGORY OF SPECIALTY OF PRACTICE Pediatric Surgery (90%): Ped Urology: VII. Ped Surg & General Surg: Ped Thoracic Surg: Specify: CURRENT PROFESSIONAL ACTIVITIES INSTITUTE A. Academic B. Hospital Appointment: Appointment: TITLE P2 AAPS VIII. IX. OTHER PEDIATRIC SURGICAL ORGANIZATIONS OF WHICH THE APPLICANT IS THE MEMBERSHIP Organizations Year of Enrollment NAMES A. & ADDRESSES OF SPONSORING MEMBERSHIPS (2) Name: Address: B. Name: Address: I HEREBY CERTIFY THAT I AM A MEMBER IN GOOD STANDING OF THE ASIAN ASSOCIATION OF PEDIATRIC SURGEONS AND THAT THE INFORMATION PRESENTED IN THIS FORM IS ACCURATE. Name Date Name X. Date SIGNATURE OF APPLICANT: (signature) (Date) Instructions to complete this form. After filling this form, please send it to your sponsoring memberships (2) to have their signatures. Curriculum vitae with bibliography should be accompanied with this form. Commending letters of sponsoring members are required. FOR AAPS OFFICE USE: APPLICATION RECEIVED BY AAPS SECRETARY SPONSORING LETTER Date RECEIVED APPROVED BY EXECUTIVE BOARD APPROVED BY COUNCIL CERTIFICATE MAILED TO APPLICANT *REGULAR MEMBERSHIP ENROLLMENT FEE ASSOCIATE MEMBERSHIP DATE RECEIVED RECEIPT#