Infection Control Measures Which Reduce Transmission of
advertisement

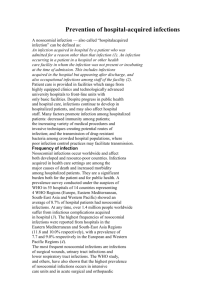
--------------------------------------------------------------------------------------------------------------------------------REPORT OF THE MONTH, Volume IV, Number 2 – March - April 2000 - - - - from the North Carolina Statewide Program for Infection Control and Epidemiology --------------------------------------------------------------------------------------------------------------------------------CONTENTS: NEWS FEATURE Institute of Medicine (IOM) Report "To Err Is Human" Active Hospital Infection Control Programs Lead to Reduced Infections REGULATORY/LEGISLATIVE Age-Specific Competencies Not Required by JCAHO QUESTION OF THE MONTH Germs from Fingernails NEWS AND ANNOUNCEMENTS COURSES FOR THE INFECTION CONTROL PROFESSIONAL NEWS FEATURE Institute of Medicine (IOM) Report "To Err Is Human" Late last year the Institute of Medicine (IOM) released a shocking report, "To Err is Human," that revealed between 50 and 100 thousand hospitalized Americans die each year due to medical errors. The IOM report spent the majority of its 300 plus pages on the problem of medication errors, but also cited health-care associated infections as a contributing factor, if not a cause, of adverse patient outcomes. Robert Gaynes, director of the National Nosocomial Infections Surveillance (NNIS) program at the Centers for Disease Control and Prevention (CDC), was quoted in a WebMD article that the IOM report defined a medical error as something preventable, a "failure of planned action," whereas nosocomial infections are adverse health events, an inadvertent consequence of medical treatment. The IOM report called for the establishment of new reporting systems to improve patient outcomes. Dr. Gaynes stated, "I think that the NNIS system is a model that would be useful for reducing adverse health events," and cites the recent MMWR (March 3, 2000) report highlighting the successes of the CDC's NNIS program for reduction of nosocomial infections. The Association for Professionals in Infection Control and Epidemiology (APIC) is working with other infection control organizations to provide a response to the IOM report. References: Institute of Medicine/National Academy of Science. November 1999. "To Err is Human." Washington, DC, NAS Press. Swint, Jean. March 2, 2000. "US Hospital Infection Rates Down Dramatically." WebMD Medical News. http://www.webmd.com Active Hospital Infection Control Programs Lead to Reduced Infections The March 3, 2000, MMWR reported on the CDC National Nosocomial Infections Surveillance (NNIS) data from the previous decade (1990-1999). NNIS used standardized data collection and analysis methods of intensive care unit (ICU) patients, the highest risk population, monitoring site-specific, risk-adjusted infection rates. During the previous decade, rates dramatically decreased for all three body sites (i.e., respiratory tract, urinary tract, and bloodstream) monitored in ICU's. Bloodstream rates decreased significantly in medical ICUs (44%), coronary ICUs (43%), pediatric ICUs (32%), and surgical ICUs (31%). Urinary tract catheter-associated infections ranged from 5.6 to 6.5 per 1000 catheter days. Central line bloodstream infections (BSIs) were highest in pediatric ICUs (7.7 BSIs per 1000 days of central line use) and lowest in coronary ICUs (4.3 BSIs per 1000 days of central line use). Ventilator-associated pneumonia (VAP) rates were highest in surgical ICUs (13.0 cases of pneumonia per 1000 days of ventilator use) and lowest in pediatrics ICUs (5.0 cases of pneumonia per 1000 days a ventilator was used). The report also summarized a survey of NNIS hospital infection control professionals (ICPs). NNIS cites the value of trained ICPs and the NNIS system as a model to prevent nosocomial infections. REGULATORY/LEGISLATIVE Age-Specific Competencies Not Required by JCAHO A facility in North Carolina was cited by Joint Commission on Accreditation of Healthcare Organizations (JCAHO) because the ICP had not been documenting age-specific competencies. However, when the national office based in Chicago was contacted by SPICE, the Associate Director, Ms. Pat Staton, stated that the infection control professional is not and never has been included in the evaluation of age-specific competence under the HR.5 standard. Ms. Stanton confirmed earlier statements made by Ms. Ann Kobs, former Associate Director of JCAHO, in the APIC Newsletter (March/April 1998). The response then and now is that ICPs serve a consultant role in the organization. The competent infection control professional is the expert on infectious diseases, regardless of age. Finally the ICP does not assess, manage, or work in areas that directly impact patients. Successful performance as an ICP is what should be evaluated. QUESTION OF THE MONTH Germs from Fingernails Q: How significant is the risk of disease transmission from fingernails? A: The Associated Press reported an outbreak of P. aeruginosa bloodstream infections in a neonatal intensive care unit at an Oklahoma City hospital (Infect Control Hosp Epidemiol 2000;21:80-85). Epidemiological evidence demonstrated an association between acquiring P. aeruginosa and exposure to two nurses. Genetic and environmental evidence supported that association and suggested, but did not prove, a possible role for long natural or long artificial fingernails in the colonization of health care workers hands with P.aeruginosa. The babies were treated in the neonatal intensive care unit and had infections caused by the same bacteria found under the nurses’ nails. Based on this and other evidence that has demonstrated a higher level of bacterial colonization under long nails (natural and artificial), UNC Hospitals has introduced a policy that restricts long nails among clinical staff in the neonatal ICU. A similar restriction exists for clinical staff who work in the Operating Room. NEWS AND ANNOUNCEMENTS On March 10, 2000, the Food and Drug Administration announced that Clinipad Corp. of Rocky Hill, Conn. was voluntarily recalling antiseptic sterile skin preparations because of a potential for bacterial contamination. For information, see the FDA web site. http://www.fda.gov/bbs/topics/NEWS/NEW00720.html The Centers for Disease Control and Prevention, Hospital Infections Program provides occasional time-sensitive e-mail messages about important healthcare events (e.g., outbreaks. product recalls) and publications (e.g., new healthcare guidelines) to persons interested in the prevention of healthcare-acquired infections and antimicrobial resistance. There is no charge for this service. For information and to sign up, see the web site. http://www2.cdc.gov/ncidod/hip/rns/hip_rns_subscribe.html COURSES FOR THE INFECTION CONTROL PROFESSIONAL "Infection Control Part II: Clinical Surveillance of Nosocomial Infections" will be held in the fall of 2000 in Chapel Hill. "Infection Control in Home Health and Hospice" will be held in the fall of 2000 in Chapel Hill. -----------------------------------------------------------------------------------------------------------------Contributors to Report of the Month: Karen K. Hoffmann, RN, MS, CIC; William A. Rutala, PhD., MPH., David J. Weber, MD, MPH, Eva P. Clontz, MEd. -----------------------------------------------------------------------------------------------------------------To subscribe to the Report of the Month, send email to spice@unc.edu Report of the Month is also available on the home page of the Statewide Program for Infection Control and Epidemiology at http://www.unc.edu/depts/spice/ The Statewide Program for Infection Control and Epidemiology (SPICE) is funded by the General Assembly of North Carolina to serve the State. SPICE is not a regulatory agency but provides education and consultation to North Carolina healthcare facilities. Copyright 2000 Statewide Program for Infection Control and Epidemiology