Lecture Notes Chapter 5 Shoulder Girdle
advertisement

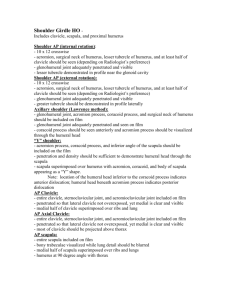
Chapter 5 Shoulder Girdle Darv Nomann R.T. (R) Les s on 1 Anatomy and Procedures of the Shoulder Girdle Shoulder Girdle Consists of Articulates with Head of humerus (shoulder joint) Manubrium of sternum (SC joint) Each other (AC joint) Functions to connect the upper limb to the trunk of the body Articulation of the upper limb with the girdle Humerus is not considered to be part of the shoulder girdle Clavicle Scapula Because the upper portion articulates with the shoulder girdle, proximal humeral anatomy is considered in evaluation of radiographs of the shoulder joint Shoulder joint Diarthrodial classification by function Synovial classification by anatomy (structure) Ball and socket type, capable of all motions Clavicle Classified as a long bone Lies just above the first rib Acromial extremity (lateral end) articulates with acromion on scapula (AC joint) Sternal extremity (medial end) articulates with manubrium of sternum (SC joint) Double curve to body Curve more pronounced in males than in females Scapula Classified as a flat bone Forms the posterior portion of the shoulder girdle Triangular in shape General Procedural Guidelines Shoulder, Proximal Humerus, AC joints, Clavicle, and Scapula Patient preparation General patient position I R s iz e SID ID markers Radiation protection Patient instructions Patient Preparation Patient preparation for shoulder girdle procedure requires removal of radiopaque artifacts from the anatomy of interest Examples: jewelry, artifacts on clothing (e.g., bra hooks, buttons) Secure all patient possessions in designated manner and location General Patient Position Shoulder procedures can be performed in erect or recumbent positions Consider patient comfort first IR Size Textbook gives most common IR sizes used for shoulder girdle procedures Collimated field generally open to size of IR SID SID is standardized as a part of procedural protocol When SID is not specified under a projection, Merrill’s Atlas recommends 48˝ (122 cm) ID Markers Consider the use of lead to absorb scatter and how it affects side marker placement Radiation Protection Shield pediatric patients and patients of reproductive age Refer to guidelines on p. 175, Volume 1 Other radiation protection measures Close collimation Optimum technique factors Patient Instructions Explain and demonstrate positions and breathing instructions Respirations suspended for most exposures Transthoracic lateral projection may use breathing technique Low mA with long exposure time Radiographic Procedures Essential Projections: Shoulder AP projections Internal rotation External rotation Neutral position Transthoracic lateral (Lawrence) Inferosuperior axial (Lawrence) PA oblique (scapular Y) AP oblique (Grashey) AP Projection in Internal Rotation Patient position Part position Rotate patient slightly toward affected shoulder Place body of scapula parallel with plane of IR Important for patients with extreme kyphosis (humpback curvature of the spine) Flex elbow slightly Rotate arm internally and rest back of hand on hip Place humeral epicondyles perpendicular to IR Central ray (CR) Perpendicular Enters patient 1˝ inferior to coracoid process AP Projection in External Rotation Patient position Part position Rotate patient slightly toward affected shoulder Place body of scapula parallel with plane of IR Important for patients with extreme kyphosis (humpback curvature of the spine Flex elbow slightly Rotate arm externally and supinate hand Place humeral epicondyles parallel to IR CR Perpendicular Enters patient 1˝ inferior to coracoid process AP Projection in Neutral Position For trauma cases If possible, have patient rest the palm of the hand against the thigh Leave arm in neutral position Places epicondyles at 45-degree angle to IR CR directed the same as for other positions Transthoracic Lateral (Lawrence) Note: Projection used for trauma patients who cannot abduct arm Patient position Supine or upright lateral Affected limb closer to IR Unaffected limb elevated over head Transthoracic Lateral (Lawrence) Part position Do not move injured limb Insure elevated shoulder is higher than injured shoulder Center surgical neck of humerus to IR Transthoracic Lateral (Lawrence) CR Perpendicular Enters midcoronal plane at surgical neck If shoulders are in same plane, CR angled 10 to 15 degrees cephalad Inferosuperior Axial Projection (Lawrence Method) Patient position Supine Head and shoulder elevated on 3˝ radiolucent support Turn head away from CR Inferosuperior Axial Projection (Lawrence Method) Part position Abduct arm to right angle If possible, place arm in external rotation Place IR crosswise on table (in a holder) centered to shoulder joint Inferosuperior Axial Projection (Lawrence Method) CR Horizontal Medial angulation of 15 to 30 degrees Enters axilla; passes through AC joint Angle depends on abduction of humerus More abduction = greater angle PA Oblique (Scapular Y) So named because when properly positioned, the acromion and coracoid process form a Y-shape Position is particularly useful to diagnose shoulder dislocations In the normal shoulder, the humeral head is directly superimposed over the junction of the Y (acromion and coracoid) Patient position Part position Upright, 45 to 60 degrees anterior oblique position Affected shoulder closer to IR Arm position is not critical Maintain patient comfort CR Perpendicular to scapulohumeral joint AP Oblique (Grashey) Patient position Part position 35 to 45 degrees posterior oblique position Affected shoulder closer to IR More rotation may be necessary if patient is recumbent Rotation should place scapula parallel to IR Head of humerus will be in contact with IR Abduct arm and slightly internally rotate Place palm of hand on abdomen CR Perpendicular to glenoid cavity Enters 2˝ (5 cm) medial and inferior to superolateral border of shoulder Radiologic Procedures Essential Projections: AC Joints AP projection (Pearson method) Patient position Part position Upright required because supine position will reduce dislocation, if present Arms hanging by side, unsupported Shoulders in same horizontal plane Separate exposures made • One without patient’s arms weighted • One with weights affixed to patient’s arms CR Perpendicular to midline of body at level of AC joints if bilateral image Perpendicular to AC joints if separate images required Radiologic Procedures Essential Projections: Clavicle AP PA AP axial PA axial Note: PA projections preferred due to reduced OID and improved image quality. AP projections used on recumbent patients. AP Clavicle Patient position Part position Upright or supine Clavicle centered to IR Arms at sides Shoulders in same horizontal plane CR Perpendicular to midshaft of clavicle PA Clavicle Patient position Part position Standing or seated upright facing vertical Bucky Center clavicle to the midline of the Bucky Arms relaxed by patient’s side Shoulders placed in same transverse plane CR Perpendicular Exits midshaft of the clavicle AP Axial Clavicle Patient position Part position Upright, lordotic position, if possible If lordotic position not possible, supine with shoulders in same plane Center clavicle to center of IR CR Lordotic position – 0 to 15 degrees cephalic Supine position – 15 to 30 degrees cephalic Amount of angle varies with patient thickness • Thinner patients = more angle Enters midshaft of clavicle PA Axial Position patient as for PA projection CR 15 to 30 degrees caudal to the supraclavicular fossa and the midshaft of the clavicle Radiologic Procedures Essential Projections: Scapula AP Lateral AP Scapula Patient position Part position Consider patient comfort first Center affected scapula to grid Abduct arm to right angle Flex elbow CR Perpendicular to point 2˝ (5 cm) inferior to coracoid process Lateral Scapula Patient position 45 to 60 degrees anterior oblique position • Posterior oblique positions can be used, but scapula will be magnified Affected scapula in contact and centered to grid Part position – to demonstrate acromion and coracoid Flex elbow and place back of hand on posterior thorax Adjust to ensure humerus does not overlap scapula OR Bring arm across anterior thorax and grasp opposite shoulder Part position – to demonstrate body Extend arm upward and rest forearm on head OR Bring arm across anterior chest and grasp opposite shoulder CR Perpendicular to mid medial border of scapula Les s on 2 Image Critique for Essential Projections of the Shoulder Girdle Shoulder Projections AP Projection in External Rotation Greater tubercle in profile on lateral side of humerus Humeral head in profile Scapulohumeral joint seen with slight overlap of humeral head on glenoid cavity Collimated field should include superior scapula, lateral half of clavicle, and proximal humerus Outline of lesser tubercle seen between humeral head and greater tubercle Soft tissue and bony trabeculae clearly demonstrated AP Projection/Neutral Position Humeral head should be seen in partial profile Greater tubercle will partially superimpose the humeral head Some overlap of the humeral head and glenoid should be seen Collimation should include superior scapula, lateral half of clavicle, and proximal humerus Soft tissue and bony details should be visualized AP Projection in Internal Rotation Collimated field includes superior scapula, lateral half of clavicle, and proximal humerus Lesser tubercle seen in profile and pointing medially Outline of greater tubercle superimposing humeral head Humeral head overlaps glenoid fossa more than in external rotation and neutral positions Soft tissue around shoulder and bony trabeculation clearly demonstrated Transthoracic Lateral (Lawrence) Proximal humerus demonstrated Scapula, clavicle, and humerus seen through lung field Scapula superimposed on T-spine Unaffected clavicle and humerus above shoulder of interest Inferosuperior Axial Projection(Lawrence) Scapulohumeral joint with slight overlap Coracoid process pointing anteriorly Lesser tubercle in profile and pointing anteriorly AC joint, acromion, and acromial end of clavicle projected through humeral head Soft tissue and bony detail demonstrated PA Oblique (Scapular Y) Scapular body should not overlap thorax Acromion seen laterally and free of superimposition Coracoid process superimposed on or slightly below clavicle Scapula in lateral profile Humeral head will be seen Superimposed on Y in normal shoulder Below the coracoid process when shoulder joint is anteriorly dislocated Below the acromion when shoulder joint is posteriorly dislocated AP Oblique (Grashey) Open joint space between humeral head and glenoid Glenoid cavity in profile Soft tissue at scapulohumeral joint Trabecular detail on glenoid and humeral head Image Critique Criteria AC Joints AP (Pearson) AC joints seen with soft tissue and without excessive density Both AC joints, with and without weights, included on one or two radiographs Patient’s body not rotated or leaning Side markers and weight or nonweight markers Separation, if present, seen on image with weights Image Critique Criteria Clavicle Projections AP/PA Clavicle Entire clavicle centered in collimated field Uniform density Lateral half of clavicle above scapula and medial half superimposing thorax AP/PA Axial Clavicle Most of clavicle projected above ribs and scapula Clavicle horizontal Entire clavicle, AC joints, and SC joints demonstrated Medial end overlaps first or second rib AP Scapula Lateral part of scapula free of superimposition of ribs Scapular horizontal and not obliqued Scapular detail seen through lung and ribs Acromion process to inferior angle demonstrated Lateral Scapula Lateral and medial borders superimposed No superimposition of scapular body on ribs Humerus does not superimposed area of interest Acromion to inferior angle demonstrated Lateral thickness of scapula with proper density