File - Wk 1-2
advertisement

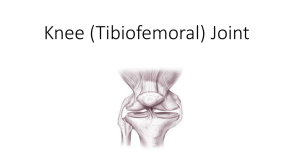
Applied Anatomy of Bones and Joints of Lower Limb Week 25 NOTE: Craig said not to worry about the foot this year – it is for second year, but I have still answered the LOs 13. The mechanism of locking and unlocking in the normal knee , in comparison to the ‘locking’ which may occur after injury - flexion and extension are the main knee movements, some rotation occurs when the knee is flexed when the knee is fully extended with the leg and foot on the ground, the knee ‘locks’ because of medial rotation of the femur on the tibia the position makes the leg a stable column and more adapted for weight bearing when the knee is ‘locked’ the thigh and leg muscles can relax briefly without making the knee joint too unstable to ‘unlock’ the knee, the popliteus contracts, rotating the femur laterally so that flexion of the knee can occur Injury - A torn meniscus can displace into the knee joint causing a mechanical block to extension and resulting in pain and muscle spasm. The classic type of meniscal tear producing a locked knee is the "Bucket Handle" tear. The torn meniscus remains attached front and back allowing the central torn portion to flip into the knee joint like the handle of a bucket. As the pain and spasm reduce the displaced meniscus can drop back allowing the knee to move freely again. This mechanical "locking" of the knee can be an intermittent feature with symptomless periods of in-between episodes. 14. The mechanism and effect of dislocation of the patella (including the factors tending to provoke and prevent recurrence) - - usually occurs laterally sue to action of quadriceps pulling along the line of the femur which is at an angle to the tibia happens more often in women due to the wider angle and relatively smaller patella the lateral dislocation is counterbalanced by the medial, more horizontal pull of the powerful vastus medialis also, the lateral femoral condyle has a more anterior projection and a deeper slope for the larger lateral patellar facet – hence a mechanical deterrent to lateral dislocation exists the stretch that occurs in the ligaments makes recurrence easier 15. The site, mechanism and diagnosis of ankle sprains - ankle sprains are tearing of fibers of the ankle ligaments nearly always an inversion injury on the weightbearing foot, the person steps on an uneven surface and the foot is forcibly inverted lateral ligament sprains occur in sports that involve running and jumping the lateral ligament is weaker than the medial and is thus more commonly injured this is due to the fact that the lateral ligament is 3 small complexes while the medial ligament is one large dand (deltoid) - many fibers of the anterior talofibular ligament (part of the lateral ligament) are torn during ankle sprains, either partially or totally, resulting in ankle instability the calcaneofibular ligament may also be torn in severe sprains, the lateral malleolus of the fibula may be fractured 16. Contrasting the medial ligament with the lateral, noting why the latter is more commonly injured - ligaments tend to tear at their weakest point - the weakest points are at or near their attachments rather than in between them - a ligament that is arranged in discrete parts, rather than a continuous band, allows more joint mobility but is weaker and is therefore more vulnerable e.g. the lateral ligament of the ankle joint - lateral ligament is 3 small ligaments; the anterior talofibular, calcaneofibular and posterior talofibular while the medial ligament is a broad deltoid ligament 17. The site, mechanism and effects of ‘flat foot’ (Pes Planus) - results from ‘fallen arches’, usually the medial parts of the longitudinal arches when a person is standing, the plantar ligaments and plantar aponeurosis stretch under the body weight if these ligaments become abnormally stretched during long periods of standing, the plantar calcaneonavicular ligament can no longer support the head of the talus the talar head displaces inferomedially and becomes prominent result – some flattening of the medial part of the longitudinal arch occurs along with lateral deviation of the forefoot 18. The mechanism and effects of hallux valgus - - Hallux valus is a foot deformity characterized by lateral deviation of the great toe (the L in valgus indicates lateral deviation) in some people the great toe overlaps the second, these people cannot move their 1st digit away from the 2nd because the sesamoids under the head of the 1st metatarsal are usually displaced and lie in the space between the heads of the 1st and 2nd metatarsals the 1st metatarsal bone shifts laterally and the sesamoid bones shift medially often the surrounding tissues swell and and the resultant pressure and friction against the shoe cause a bursa to form when tender and inflamed, the bursa is called a bunion 19. The mechanism and effect of ‘anterior compartment syndrome’ (of the leg) - - the septa forming the boundaries of the leg are strong, therefore trauma to muscles in compartments may cause haemorrage, oedema and inflammation of the muscles with arterial bleeding, the pressure may reach levels high enough to compress structures in the compartments concerned structures distal to the compressed area may become iscaemic, and permanently injured – i.e. loss of motor function on muscles whose blood supply and/or innervation is affected loss of dital pulses is an abvious sign of arterial compression as is lowering of the temperature of tissues distal to the compression a fasciotomy (incision of a fascial septum) may be performed to relieve the pressure in the compartment concerned