Case 2
advertisement

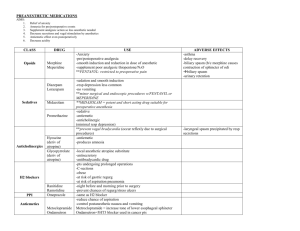
Chapter 16: General Anesthetics Case Study 2 GB is a 75-year-old male, who sustained a severe hip injury while bone-fish fishing off the Florida Keys. He is presently in the hospital where you are the chief pharmacist and will be undergoing hip repair surgery requiring general anesthesia. GB is aging gracefully and is in generally good health for his age. His blood pressure is normal (120/80 mm Hg) with no history of cardiovascular problems. His creatinine clearance is 125 ml/min, which is normal for his age. GB is currently taking diazepam (Valium, structure 5) for chronic back pain. Evaluate structures 1–4 for use as the general anesthetic for GB’s surgery. 1. Identify the therapeutic problem(s) where the pharmacist's intervention may benefit the patient. GB is a geriatric patient, who will undergo hip repair surgery. A general anesthetic is required that is appropriate for a patient who is 75-years-old. Although his health is normal for his age, geriatric patients have decreased kidney and liver function, which affect the rate of metabolism and excretion of drugs. It is important to keep this in mind when administering medication, including anesthesia. 2. Identify and prioritize the patient specific factors that must be considered to achieve the desired therapeutic outcomes. GB is 75-year-old male who has suffered a hip fracture. GB will undergo hip repair surgery requiring general anesthesia. GB is in generally good health for his age but is taking Valium for chronic backache. 3. Conduct a thorough and mechanistically oriented structure-activity analysis of all therapeutic alternatives provided in the case. Structures 1 and 2 are volatile anesthetics and structures 3 and 4 are parenteral anesthetics. They can be used alone or the parenteral anesthetics can be used to induce anesthesia and then the volatile anesthetics used to maintain anesthesia during the surgical procedure. Structure 1 is a halogenated ethane and the only useful halogenated hydrocarbon general anesthetic. It has a blood/gas coefficient of 2.30 and a MAC of 0.77. It has a rapid onset/recovery when used alone or with nitrous oxide. It is subject to spontaneous oxidation to HCl, HBr, and phosgene and is, therefore, stabilized with thymol and dispensed in amber bottles. Twenty percent of the administered dose is metabolized to oxalic acid and hydroxyacetic acid, which accounts for its hepatotoxicity. Structure 1 attenuates ventilation parameters by interacting with carotid and central chemoreceptors. These receptors are already attenuated in the elderly patient. Structure 2 a halogenated methyl ethyl ether and can be considered an isoflurane analog. It has a blood/gas coefficient of 12 and a MAC of 0.16. Therefore, it has a high solubility in blood, giving it a slow onset/recovery. Its MAC is the lowest of the halogenated anesthetics making it the most potent. Fifty percent of the administered dose is metabolized characterized by having the highest rate of fluoride ion production, hence the greatest risk for nephrotoxicity. Drug metabolism is compromised in the elderly because of the normal aging process that results in decreased activity of some hepatic enzymes as well as decreased numbers of hepatocytes and decreased perfusion. Structure 3 is 2-(o-chlorophenyl)-2-methylamino-cyclohexanone and is structurally related to PCP (phencyclidine). It is a short-acting parenteral anesthetic that doesn’t relax skeletal muscle. Recovery from anesthesia may be accompanied by “emergence delirium” and vivid dreams can occur for up to 24 hours after administration. It is metabolized by CYP 450 mediated Ndemethylation to an active metabolite. It is also metabolized by cyclohexane ring hydroxylation. It has one asymmetric center and the S (+) isomer has been shown to be 3–5 times more potent as an anesthetic. However, it is used as the racemic mixture. Structure 3 is believed to produce anesthesia by blocking the NMDA+ controlled K channel on excitatory synapses on pyramidal cells. Structure 4 is 2,6-diisopropylphenol. It has a rapid onset (1 minute) and short duration of action (5 minutes). Sustaining anesthesia requires continued dosing or use of a volatile anesthetic. Structure 4 acts by enhancing the GABA-ergic system in the CNS at the benzodiazepine receptor but not binding to the same site. More than 99% of the administered dose is metabolized, primarily to glucuronide and sulfate conjugates. Structure 4 administration lowers blood pressure and slows heart rate and dosage should be carefully adjusted in the geriatric patient. 4. Evaluate the SAR findings against the patient specific factors and desired therapeutic outcomes and make a therapeutic decision. Structure 1 (halothane) would not be an appropriate anesthetic to be used in this case. Its chemoreceptor impairment will enhance the already age-compromised ventilation in geriatric patients. In addition, hypotension and decreased cardiac output may occur if the patient is induced with ketamine and maintained with halothane. Structure 2 (methoxyflurane) would be the least likely anesthetic to be used in this case. Its slow onset and recovery and its high rate of metabolism to toxic products make it well known as a hepatotoxic and nephrotoxic agent. It would especially be difficult to use in the geriatric patient who normally has decreased liver and kidney function. Structure 3 (ketamine) would be a good choice in this case. It has less cardiovascular effects and can actually slightly raise blood pressure and heart rate. It can be used alone but would be better used to induce anesthesia and with anesthesia being maintained with a rapid-acting volatile anesthetic such as desflurane that has minimal metabolism and minor nephrotoxic effects. In addition, it can be used along with Valium since they have different mechanisms of action. Structure 4 (propofol) would not be a good choice here either for induction of anesthesia for use alone. It lowers blood pressure and slows the heart and requires extensive metabolism for termination of action. In addition it is synergistic with Valium (benzodiazepines) and would only complicate the administration of anesthesia in this patient. 5. Counsel your patient. Tell GB to divulge all medications to his physicians, especially if he is taking herbals because of possible herb anesthetic interactions. GB will be groggy and may experience slight nausea and vomiting as well as some postoperative chills. GB may experience bad dreams for a day or two after surgery if ketamine was used to induce or maintain anesthesia.