Anesthesia Management Plan
advertisement

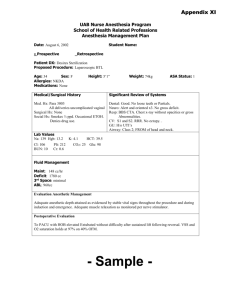
Appendix XIa UAB Nurse Anesthesia Program School of Health Related Professions Anesthesia Management Plan Date: August 6, 2002 __Prospective Student Name: x _Retrospective Patient DX: Hemorroids Proposed Procedure: Hemorrhoidectomy Age: 40 Sex: M Allergies: NKDA Medications: None Height: 5’10” Weight: 84kg ASA Status: 2 Medical/Surgical History Significant Review of Systems Med. Hx: Left foot fracture, hemorrhoids Surgical Hx: Hemorrhoidectomy ’94 with GA NAC Social Hx: Smokes ½ ppd, denies ETOH, H/O cocaine use. Works as a furniture mover. Dental: Intact Neuro: No gross deficit Resp: BBS CTA CV: S1 and S2 with RRR. Normal heart sounds. No 12 lead ECG recorded. Airway: Class 1 FROM head and neck. Lab Values Hct: 46 Hgb: 16 Fluid Management Maint: 170 cc/hr Deficit: 2040cc 3rd Space: 84 cc/hr ABL: 1260cc Evaluation Anesthetic Management Spinal Anesthetic Block used for this procedure. T4 level assessed at onset of procedure. No complications with ventilation or hemodynamics intraop. Postoperative Evaluation Level of block receded to T7 upon transfer to PACU. All VSS. No c/o pain or shortness of breath. - Sample - Scheduled Procedure: Hemorrhoidectomy Position: Prone jacknife in this instance Exposure: Anus and surrounding perineum. Incision: A series or longitudinal incisions is made from the anal verge to the top of the anal columns Blood bank: No order necessary usually EBL: < 100cc Surgical time: 45-90 minutes Nerves: Pudendal Nerves Overview Hemorrhoids are naturally occurring tissues made up of venous vasculature that protrude into the rectal and anal lumens sometimes can become incarcerated externally. The primary symptoms are pain and bleeding. The primary reason for the manifestation of hemorrhoids is degeneration of the structures that support them. The surgical correction involves insertion of an anoscope and grasping and excision of the hemorrhoid deep to the natural plane of the hemmorrhoidal tissue. All redundent tissue is removed and the tissue is closed making sure that enough mucosa is left between adjacent hemorroidal columns. The majority of hemorrhoidectomies are performed with local anesthesia unless specifically requested by the patient. Pre-op Assessment . Resp: Careful assessment of the respiratory system is required. Any h/o COPD or decreased respiratory reserve should be noted. CV: Usual assessment of CV status including h/o HTN, CAD, MI etc. Neuro: Assessment for gross deficit required. GI: Assess for h/o constipation and other GI disturbances. Labs: H & H unless history indicates otherwise. PreMeds: 10mg Reglan and 300mg Tagamet po Anesthesia Implications If pt. has limited ventilatory reserve as with COPD, lithotomy position may be tolerated better than prone jacknife. If considerable pain is associated with sitting then spinal may be performed in the lateral decubitus position. If pt is on ASA, NSAIDS or dipyridamole, PT/PTT may be needed prior to performance of regional anesthesia. Chest rolls will be needed to maximize chest expansion while in jacknife position and genitalia need to be checked for pinching in the bed as well as padding all pressure points in the lower and upper extremities. Adequate preload with a good large IV should be given prior to injection of intrathecal LA to avoid hypotension and bradycardia. The level of the block should be monitored closely and communication with the patient should be continuous as respiratory distress and agitation may result if the block extends into the upper thoracic or lower cervical level. Nausea is common with blocks that cause significant hypotension. Ephedrine should be readily available and not withheld if signs of hypotension are present. Anesthetic Management 1mg Versed prior to SAB. Sat up for procedure. Back prepped x 3 and allowed to dry. Local anesthetic SQ at L2-3. #25g Whitacre through introducer without difficulty at L2-3 to LOR and +CSF return. No blood aspirated or paresthesia elicited. 2cc 5% Lidocaine with 20mcg Fentanyl intrathecal without difficulty and + CSF return. Pt carefully prone with all pressure pts. checked and ok. Genitalia checked and ok. T4 level assessed at onset of surgery. Pt placed on 3L nc O2and 80mcg of Fentanyl were given prior to start of surgery. Pt. without complaints during procedure.