Pre-operative work up for trauma patients
advertisement

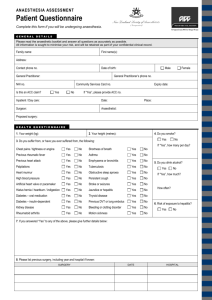
The A to Z of anaesthesia for elderly trauma patients PLEASE NOTE:- these guidelines are not applicable to patients coming for elective surgery. Anaesthetists who regularly give anaesthetics for trauma lists have prepared this document. If you work within these guidelines, patients will usually be accepted for theatre. The judgement of the anaesthetist on the day over rides anything written here. In particular, if less experienced anaesthetists are working on their own, patients may still be turned down. Evidence suggests that reduced time to surgery correlates well with increased survival. YOU can make the difference! Atrial Fibrillation All patients in AF should have a ventricular rate of less than 100. Regular nursing observations should include the rate counted at the apex beat, not peripherally. If control is poor: Exclude or treat factors that may lead to new or fast AF. Check potassium and magnesium levels. Consider hypovolaemia, sepsis, pain, hypoxaemia. Trust guidelines suggest the use of beta blockers. Please consider contraindications to treatment before prescribing. If in doubt, ask *. For previously undiagnosed AF, we suggest that intra-venous digoxin gives a reliable effect within 4 – 6 hours. If you are unsure about the dose, please ask *. For patients already on treatment for AF, you should consider exacerbating factors as above, and then discuss increased treatment with the orthogeriatricians. If the rate is between 100 and 120, it may be possible to proceed – please discuss with the anaesthetist. If the rate is over 120 more treatment is usually required. Blood tests All elderly trauma patients need FBC and Coag, U&E, LFT AND we need the results in the notes by 8 am on the day of surgery! G&S – all #NOF, all nailings, major joint replacements or revisions, all #long bones Cross match – only for patients who are highly likely to need blood. We can get blood on a G&S in about 15 minutes. If you are not sure ask a surgeon or anaesthetist. And ALSO:RECHECK the U&E as follows: every 48 hours if it was normal on admission daily if it was abnormal on admission or at any stage Chest Infections Chest infection is rarely a reason to cancel a case. Antibiotics should be started promptly. Delaying surgery to allow a chest infection to improve is usually futile as chest infections get worse, not better in the presence of a #NOF. Patients with a chest infection can usually have a spinal anaesthetic. Exceptions to this are : raised INR (more than 1.5) rods or other instrumentation of the spine patient too breathless to tolerate lying at about 20 degrees from flat severe aortic stenosis or critical coronary artery disease Please let the anaesthetist know if a patient with a chest infection also has one of these conditions. Patients with chest infections should be listed for the next available daytime slot. Chest X-Ray All patients with #NOF should have a chest X ray on arrival. A supine AP film is satisfactory. Anaesthetists particularly value a chest X Ray for the information it gives about the mediastinal shadow and heart size. Information about the lungs is less useful because clinical impression is more important than the CXR appearance. A repeat X Ray to assess a chest infection is rarely of any use. Creatinine If the creatinine is >200, this may be a very significant elevation in a small elderly person. It may not prevent the patient going to theatre, but we will need some additional information. Please seek old results. If new seek the cause. Ensure hydration and not in retention. Start a fluid balance chart. Diabetes Detailed guidelines for diabetes are found in the Trust protocol. Most trauma patients can eat and drink within 4 hours after surgery and plans for control of diabetes should take this into account. Insulin dependent patients need to be placed first on the operating list. They usually need a dextrose and insulin regime started on the morning of surgery. Non insulin dependent patients do NOT usually need a dextrose and insulin regime pre-op. They should be placed as early as possible on the list, fasted, and diabetic tablets omitted. The blood sugar should be monitored 1-2 hourly. If it rises above 11 you may need to use insulin. Discuss with orthogeriatricians or the anaesthetist. Diet controlled diabetics almost never need a dextrose and insulin regime pre-operatively. Their blood sugar should be monitored. High blood sugars are not usually a reason to delay surgery in urgent trauma patients, unless the patient is ketotic and dehydrated. You should start treatment urgently however and discuss what you are doing with the anaesthetist. ECG ALL elderly trauma patients need an ECG. The following rhythms are of interest: Atrial fibrillation – see earlier note Tri-fascicular block. Discuss with cardiology or senior trauma anaesthetist ASAP. Complete heart block. Discuss with cardiologist or senior trauma anaesthetist ASAP. Multiple or multi-focal ectopics, bigemini or trigemini. If no history of blackouts – ensure normal K+, check and correct Mg++. If history of blackouts – discuss with orthogeriatrics, cardiology or senior trauma anaesthetist ASAP. Echo (These remarks should not be applied to pre-assessment for elective surgery. ) There are two reasons that an anaesthetist may be require an echo: to find the origin of a heart murmur (most importantly to exclude aortic stenosis) to establish LV function Murmurs Pan sytolic murmurs heard at the apex (mitral regurgitation). These do not need an echo. Ejection systolic murmurs heard in the aortic area - ONLY need an urgent echo IF there is evidence that there may be significant aortic stenosis. This is indicated by two or more of the following, (or one of the following if severe): history of angina on exertion unexplained syncope or near syncope slow rising pulse clinically (try the brachial pulse for this) absent 2nd heart sound LVH on the ECG without hypertension CXR suggests AS (enlarged heart, post stenotic dilation of aorta) LV function If the patient is known to have heart failure, we do NOT need an echo – we will treat as reduced LV function. If the patient is breathless at rest or on low level exertion, the anaesthetist will need to work out whether this is due to LV failure or lung disease. If he/she cannot make this diagnosis on clinical grounds, an echo may help. These patients should be reviewed by an orthogeriatrician or senior anaesthetist as soon as possible after admission. Please arrange the echo by contacting Sandra Wheeler on 6573. All echos requested pre-operatively must be done the same day. If an echo request appears to be delaying surgery, please rediscuss the need for it with a senior trauma anaesthetist. Haemoglobin We recommend the following guidelines for elderly trauma patients: If Hb is <9g/dl please transfuse up to 10g/dl. If Hb is 9 – 9.9g/dl and there is a history of ischaemic heart disease, please transfuse up to 10g/dl. If Hb is 9 – 9.9 and there is no history of ischaemic heart disease, please order 2 units of blood to be available in theatre. If transfused there must be a post transfusion check Hb available. Heparin Sub cutaneous heparin should be prescribed as in your department guidelines. This is currently Tinzaparin 4500 units. Always prescribe LMWH to be given between 18:00 and 20:00. This is because we cannot do a spinal anaesthetic within 12 hours of a dose. The evening dose allows us to do a spinal at any time during the next day’s list. INR The INR should be below 2 for most operations. For a spinal anaesthetic the INR must be less than 1.5 For patients on warfarin, please use the flowchart below: INR 2-6.5 Low risk patient AF Recurrent DVT/PE DVT/PE>3 months Thrombophilia High risk patient Prosthetic Heart Valves Caval Filters DVT/Pe<3 months Tinzaparin s/c after 4 hours Vit K 1mg CHECK INR at 7am Start IV heparin <1.5 INR >6.5 Call haematologist of the week 1.5-2.5 >2.5 2 units FFP before surgery Proceed with surgery Restart Warfarin 24 hours post surgery, and discontinue heparin when INR is therapeutic. Intra-venous infusion All #NOF patients need an IVI. U&E should be monitored alternate days or daily if abnormal. Pacemakers A pacemaker check should usually be requested pre-op, especially if the fall is unexplained. It also helps us to know the type of pacemaker and the patient’s unpaced rhythm. Please contact the pacemaker service on 6636 within normal office hours, explaining that the patient requires emergency surgery. Platelet count If the platelet count is >120, no action is required. If the platelet count is 80 – 120 this should be followed up after surgery. It may need investigating. If the platelet count is 50 – 80, this will usually exclude a spinal anaesthetic. The surgeon is likely to want platelet cover, which should be planned in advance with the haematologist. Ask the lab to do a blood film – platelets may clump, which can give a misleading low result. If the platelet count is below 50, this should be discussed with the haematologist of the week. Potassium Potassium level must be > 3 mmol/dl, or the case will be cancelled. If the potassium level is between 3 and 3.5, we will accept only if adequate potassium replacement is in progress. If the potassium is less than 3.5 there must be a daily check until it comes up and the cause has been stopped/treated. Remember you can get an instant potassium from the blood gas machine (take a heparinised venous sample) Consider why the potassium is low, and treat the cause. Sodium Patients with low sodium may have impaired control of sodium and water balance in the brain. This may lead to cerebral events (including fits, brain swelling and brain damage). Also note Slow onset or chronic hyponatraemia may be compensated and safe. Rapid correction can be unsafe. Na+ 120 – 130 : Find previous Na+ results if available. Consider cause. Stop inappropriate diuretics. Avoid IV dextrose. We may accept, especially if evidence that it is chronic. If it has fallen over a short time (a few days) we may postpone surgery. Please check urine and plasma osmolality, remove the cause if known and contact the orthogeriatrician. Do not try and give large amounts of sodium. Na+ <120 – all of the above plus seek orthogeriatric opinion. Thyroid function tests These should be done on admission in patients on thyroxine. However if the patient is clinically euthyroid, we will usually accept the patient for theatre without a result. And finally:Special Anaesthetic review Please note we will always want to be warned about patients as follows: History of difficult intubation; anyone who can’t open their mouth; anyone with restricted neck movement (eg Ankylosing spondylitis) or unstable neck (# or RA) Known problems with GA – malignant hyperpyrexia, suxamethonium apnoea, any unplanned ICU admission in the past Notes Notes Notes ! If your patient has had relevant treatment which is documented in other notes – please get those notes. If the notes are not available, please ask the GP to fax a copy of their patient summary. *Contact Details Orthogeriatrician insert contact no Trauma Coordinator insert contact no Trauma theatre insert contact no Anaesthetic Consultant insert contact no Cardiology SpR insert contact no Medical SpR (ward cover) Contact switchboard for bleep number Haematologist of the Week Contact switchboard for number