Strengthening Health Systems through the
Nigerian Ministry
of Defense—U.S. Department of Defense
Walter Reed Program Nigeria Partnership
Nelson L. Michael, M.D., Ph.D
Colonel, Medical Corps, U.S. Army
Director
US Military HIV Research Program (MHRP)
Walter Reed Army Institute of Research
2012 USPHS Scientific and Training Symposium
The views expressed are those of the presenter and should not be construed
to represent the positions of the U.S. Army or DoD
1
20 June 2012
2
20 June 2012
Towards a Globally Effective HIV Vaccine:
The role for Nigeria
3
20 June 2012
MHRP’s Product Development Plan
MHRP’s vaccine development strategy emphasizes regional
and global approaches.
1
BUILDING ON RV144
REGIONAL VACCINE STRATEGY
Building on the RV144 outcome and lessons learned,
conduct efficacy trials of the prime-boost concept in:
a) Thai MSM populations
b) High-risk populations in Southern Africa
2
DIVERSIFYING AND REFINING THE PORTFOLIO
GLOBAL VACCINE STRATEGY
Pursuing diverse platforms (e.g. vectors, multivalent constructs or mosaic inserts) that build on
the prime-boost concept and readily translate to
multi-clade testing and a globally effective vaccine.
4
4
20 June 2012
Pox-Protein
5
20 June 2012
NEJM 361:2209 (03 Dec 09)
6
20 June 2012
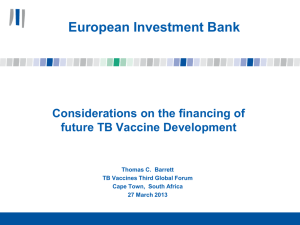
RV 144 demonstrated efficacy
for HIV acquisition
C. Modified Intention-to-Treat Analysis*
1.0
0.9
Placebo
Probability of HIV Infection (%)
0.8
0.7
0.6
0.5
Vaccine
0.4
0.3
0.2
0.1
0.0
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Years
N=16,395
51 vaccine, 74 placebo HIV infected
Est. VE = 31% 95% CI 1-51% (p=0.04)
7
Rerks-Ngarm et al. (2009, NEJM)
20 June 2012
What we have learned—RV 144
Protection among low incidence heterosexual Thais, VE 31.2% at
42 months
No effect on post-infection viremia or CD4 count
Relatively monophyletic circulating variants CRF01_AE
Efficacy appears to be early and non-durable
Evoked binding Ab but not measurable, primary isolate Nab— BAb
appeared early and decreased by > 10 fold over 6 months
CD4+ Env responses, but not CD8 responses
Correlate/surrogate studies limited by samples and endpoints
8
20 June 2012
What we would want next
Extend the observation of early 60% efficacy by increasing
the durability of such protection (additional boosts)
Heterosexual risk groups in Asia
Ensure that we can elucidate correlates/surrogates of
protection with more appropriate sample collection.
Establish protection in higher incidence populations
(additional boosts)
9
Heterosexuals in sub-Saharan Africa
MSM in Africa and Asia
20 June 2012
NEJM 366:1275 (05 Apr 2012)
10
20 June 2012
Comparison of Infection Rate and Vaccine Efficacy
Between Vaccine and Placebo Recipients in the RV144
ALVAC-HIV, AIDSVAX B/E Trial
V1V2 Antibodies
High V1V2
Antibodies,
Increased
Vaccine Efficacy
Low V1V2
Antibodies,
Same Infection
Rate as Placebos
11
20 June 2012
Comparison of Infection Rate and Vaccine Efficacy
Between Vaccinees and Placebo Recipients in the RV144
ALVAC-HIV, AIDSVAX B/E Trial
IgA Magnitude and Breadth Antibodies
High IgA
Antibodies,
No Efficacy,
Same Infection
Rate as
Placebo—No
Enhancement
Low IgA,
Increased
Vaccine Efficacy
12
20 June 2012
Sequence variation in position 169
Edlefsen, SCHARP
13
20 June 2012
Sequence variation in position 181
Edlefsen, SCHARP
14
20 June 2012
Summary
The case control correlates data suggest 2 hypotheses:
Binding to gp70:V1V2 correlates inversely with HIV infection
rate?
•
•
15
A244 and MN V2 crown linear peptides show similar effects
Linear epitope microarray data suggest V2 effect
Anti-Env IgA M-B correlates directly with HIV infection rate
Sieve analysis suggests a V2 effect
20 June 2012
Planned studies are mutually reinforcing and will
amplify public health impact and regional relevance.
Precedent
for vaccine
efficacy
RV144
Focus on
regional
public health
impact
THAILAND
High Risk MSM
Mutually reinforcing
studies strengthen and
support public health
benefit in target
populations and the
translation of the
platform globally.
Future amplification
of global reach
US/EUROPE
SOUTHEAST ASIA
SOUTHERN
AFRICA
Republic of South
Africa (RSA)
High Risk
Heterosexual
Strategy for achieving potential licensure in target markets and having the
broadest public health impact.
16
16
May 2011
20 June 2012
The pox-protein approach is regional
Will we have to tailor vaccines for multiple sub-epidemics?
What will be the inducement to industry to support such
an approach?
There are significant public health challenges with regional
vaccine approaches.
What about Nigeria, and the rest of West Africa, with a
dominance of pure subtype G and A/G recombinant HIV
infections?
Can we make a universal HIV vaccine?
17
20 June 2012
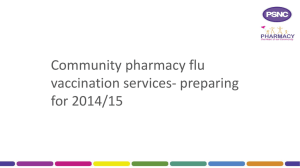
Ad26-MVA +/- protein
Barouch et al Nature 482:89-93 02 Feb 2012
18
20 June 2012
Nature 482, 89–93 (02 February 2012)
100
% Uninfected
80
DNA/MVA
60
MVA/MVA
Ad26/MVA
40
MVA/Ad26
20
Sham
0
0
2
4
6
8
Number of IR Challenges
19
19
20 June 2012
MVA/Ad26 and Ad26/MVA Regimens Lower Early Setpoint Viral
Loads Following SIVmac251 Infection
9
Sham
8
8
7
7
9
MVA/MVA
418-08
8
419-08
7
420-08
6
6
422-08
5
5
423-08
4
4
5.75
3
3
2
2
0
20
40
60
80
100
424-08
Days Following Infection
446-08
5
447-08
5.47
448-08
449-08
3
2
MEAN
20
40
60
80
100
450-08
MEAN
0
20
Days Following Infection
9
40
60
80
Ad26/MVA
426-08
3x resistance to infection
409-081 log
4/8 : viremia blunted
410-08
3/8 : rapid virologic
control
411-08
1/8 : persistently uninfected
8
8
7
7
6
6
443-08
412-08
5
5
444-08
413-08
434-08
442-08
4.55
4
452-08
4
3.83
453-08
3
3
2
2
20
40
60
80
Days Following Infection
100
454-08
414-08
416-08
417-08
MEAN
0
100
Days Following Infection
9
MVA/Ad26
0
20
441-08
6
4
435-08
0
DNA/MVA
440-08
445-08
6.09
425-08
Log SIV RNA
Log SIV RNA
9
MEAN
20
40
60
80
100
Days Following Infection
20 June 2012
Protection Against Acquisition of IR SIVmac251 by
Ad35/Ad26-SIVsmE543GagPolEnv Vaccine
100
GagPol (N=16)
GagPolEnv (N=16)
% Uninfected
80
Sham (N=8)
60
40
20
0
0
2
4
6
Number of IR Challenges
21
20 June 2012
Ad26-MVA correlates analysis
•
•
22
Acquisition endpoint.
•
envelope binding antibody r= .79 p<.0001.
•
neutralization antibody r=.50 p=.0034
•
ADCC r=.38 p=.034
set point viral load endpoint, Many correlates (N=27);
•
prechallenge gag elispot count and gag elispot breadth
were both correlated (r=-.50 p=.006 and r=-.64 p=.0002,
respectively) with the endpoint.
•
peak envelope binding antibody r=-.70 followed by
prechallenge neutralizing antibodyr=.67.
20 June 2012
Increment 2: Pathway to a Global HIV Vaccine
Phase I:
Safety and
immunogenicity
Trials are
prime-boost
regimens
with
additional
protein
boost based
on RV144
data
Multi-clade (A/C/E) or mosaic (M1/M2) inserts
Phase IIa: DNA/MVA vs
Ad26/MVA (Ad35) for
epitope and clade breadth
and magnitude of immune
response
Phase IIb
Efficacy#:
2011
2012
2013
2014
2015
2- or 3-arm
efficacy trial with
common placebo
group
2016
2017
A successful outcome will yield a mosaic or multi-clade vaccine effective in
high-risk populations. Commercial partners have yet to be identified and may
restrict development and access to products.
23 23
.
20 June 2012
How to prepare Nigeria for HIV vaccine
studies?
24
20 June 2012
Preparing Nigeria for HIV Vaccine Development
Recognize a public health gap—Feb 2004
Take risk—July 2004
Recognize that you are in someone else’s country
and never forget it—Jan 2005 (Bolingo)
Develop durable and inclusive frameworks
(steering committees, EPIC)
Deliver prevention, care and treatment first
(PEPFAR)
25
20 June 2012
Preparing Nigeria for HIV Vaccine Development—2
Find champions (Drs. Orits, Njoku, Idoko)
Give the champions protegees—Jide, Ayemoba,
Umar
Build a laboratory that serves service delivery,
then research (Mogadishu)
Assess risk, prevalence and subtypes (RV 230)
Community engagement from the inception (GPP
version 2.0)
26
20 June 2012
Preparing Nigeria for HIV Vaccine Development—3
Work with partners (IHV, Harvard, Pop Council,
Heartland Alliance, CDC, USAID, etc)
Focus on key populations—MSM, CSW (high
incidence)
Engage with major stake holders (NIH, Gates) but
do not vex them….let them see you take risk
Advocate…UNAIDS, AVAC, AAVP
South-south partnerships within MHRP
27
20 June 2012
28
20 June 2012
Acknowledgements
Supported by:
Collaboration for AIDS Vaccine Discovery Grant From the Bill and Melinda Gates
Foundation
HVTN, DAIDS, NIAID
With Collaborations with the MHRP and Thai Ministry of Public Health
National Institute of Allergy and Infectious Diseases (NIAID)
National Institutes of Health (NIH)
Division of AIDS (DAIDS)
U.S. Department of Health and Human Services (HHS)
Center for HIV/AIDS Vaccine Immunology (CHAVI) # U19 AI067854-06
HVTN
29
20 June 2012
 0
0