ATN - Nephrology
advertisement

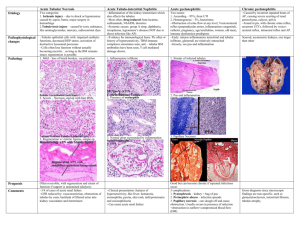
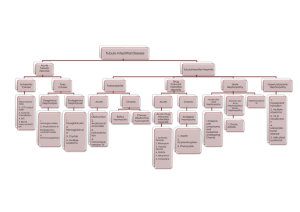
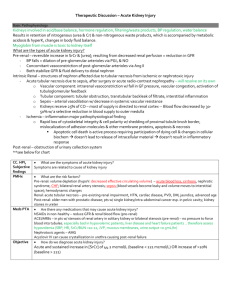
Acute Tubular Necrosis Douglas Stahura D.O. Grandview Hospital 7/24/2002 Causes of Acute Renal Failure Pre-renal Renal parenchymal (intrinsic) Post-renal Acute Tubular Necrosis (ATN) Pre-renal azotemia and ATN are a spectrum of manifestation of renal hypoperfusion Pre-renal – mild to moderate ischemia ATN – severe/prolonged ischemia with injury to parenchyma which does not resolve immediately with restoration of renal perfusion Describes the renal parenchymal injury following renal ischemia OR exposure to nephrotoxins, which particularly injure the tubular epithelium Acute Tubular Necrosis (ATN) What segments of the nephron? Why? How to recognize – clinical/histological Pathophysiology Ischemia/toxins Clinical course Acute Tubular Necrosis (ATN) Site of tubular injury Proximal tubule (S3, pars recta) Medullary thick ascending limb Medulla receives 20% of total renal blood flow Intense metabolic activity O2 supply/demand balance is delicate Multiple causes of cell injury Acute Tubular Necrosis (ATN) Causes of cell injury Endothelin/Nitric Oxide balance Endothelin(ET-1 isoform) potent vasoconstrictor produced in renal endothelium, epithelium, mesangium Nitric Oxide potent vasodilator produced in endothelium ATP Depletion Cell Swelling Acute Tubular Necrosis (ATN) Causes of cell injury Intracellular Calcium increases Intracellular acidosis Oxidant injury Inflammatory response from ischemia/reperfusion Acute Tubular Necrosis (ATN) Tubular Injury Cell swelling, vacuolation, apical blebbing, loss of brush border, loss of cell polarity, necrosis, sloughing Acute Tubular Necrosis (ATN) Histopathology Acute Tubular Necrosis (ATN) Nephrotoxins Endogenous – myoglobin, hemoglobin, light chains, Crystals, Hypercalcemia Exogenous – ethylene glycol, IV contrast, Medications: Aminoglycosides, Acyclovir, Methotrexate, Amphotericin B, Cisplatin, Ifosfamide, Foscarnet Acute Tubular Necrosis (ATN) Clinical Course Initiation phase Maintenance phase GFR = 5-10 ml/min Lasts weeks to months Recovery phase Heralded by increase of urine output Acute Tubular Necrosis (ATN) Diagnostics FENA >1% Una > 40 Meq/dL Uosm < 350 mosm/dL Renal Ultrasound – normal size Urine microscopic – “muddy brown cast” Acute Tubular Necrosis (ATN) Outcomes Mortality about 50% Acute Tubular Necrosis (ATN) Treatment Supportive – maintain pt non-oliguric for ease in fluid balance/management Maintain perfusion of kidneys MAP=65 Treat underlying illness/interrupt insult Acute Tubular Necrosis (ATN) Review Caused by severe hypoperfusion/toxin Parenchymal injury that is not immediately reversible Effects the proximal and mTAL epithilium Hallmark “muddy brown casts” No specific treatment/remedy Mortality 50% References The Kidney 6th Edition, Brenner and Rector Comprehensive Clinical Nephrology, Johnson Clinical Physiology of Acid-Base and Electrolyte Disorders, Rose