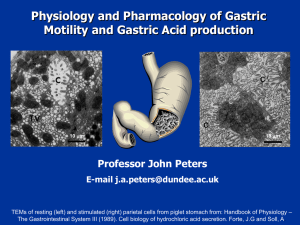
Pathogenesis of peptic ulcer
advertisement

Chapter 32 drug used in digestive system This chapter describes drugs used to treat these common medical conditions involving the gastrointestinal tract: peptic ulcers, dyspepsia, vomitting, diarrhea and constipation, etc. Part Ⅰ Drugs Used in Peptic Ulcer peptic ulcer A benign, localized defect in the mucosa of any part of the gastrointestinal tract. duodenal ulcer gastric ulcer [Symptoms and complications] • The most important symptom is abdominal pain and discomfort. The atypical symptoms are abdomen distention, inappetence, belching, reflux of gastric acid. • The severe complications are hemorrhage, perforation, obstruction and canceration. [Pathogenesis of peptic ulcer] • although the pathogenesis of peptic ulcer disease is not fully understood, the theory that the balance between mucosal defense and injury is broken are recognized. [Pathogenesis of peptic ulcer] 1. Aggressive factors↑ Helicobacter Pylori ( H. Pylori) gastric acid and pepsin 2. Defensive factors↓ mucus-bicarbonate barrier prostaglandins Helicobacter Pylori ( H. Pylori) In 1983, H. pylori was found by two Australians, Marshall and Warren. Now, it is believed that H. pylori is the most important pathogenic factor to peptic ulcer. “No H.P., no ulcer.” And the two men won the noble prize for the important findings in 2005. H. Pylori (×48,000) flagellum H. Pylori on gastric mucosa (×16,000) Actions of H. Pylori gastric acid and pepsin Pepsin can decompose protein molecule. But its activity is depended on the pH value. When local pH value elevates to 4, pepsin can’t work well. Gastric acid is the key-factor of the formation of peptic ulcer. we can also say that “No acid, no ulcer.” mucus-bicarbonate barrier • The epithelial layer of the mucosa is composed of tightly adjoined cells that are specialized for existence in an acid medium. Their tight junctions, synthesis of PGs and secretion of mucus and bicarbonate all contribute to maintenance of the epithelial barrier. mucus-bicarbonate barrier mucus Prostaglandins(PGs) Prostaglandins are thought to enhance resistance to injury by maintaining blood flow to the mucosa. Thus it also plays a major role in the maintenance of defensive mechanism. Classification of drugs : Ⅰ.Antacids Ⅱ.Agents decreasing secretion of gastric acid Ⅲ. Agents protecting mucosal barrier Ⅳ.Agents eradicating helicobacter pylori Ⅰ Antacids • Have been used for centuries in the treatment of patients with acid-peptic disorders. • Were the mainstay of treatment for acidpeptic disorders until the advent of H2receptor antagonists and proton pump inhibitors. Ⅰ Antacids weak bases : Mg(OH)2 , Al(OH)3 , CaCO3 , NaHCO3 actions: 1) prevent injury from H+ 2) neutralize gastric acid → reduce gastric acidity→ reduce peptic activity 3) protect face of ulcer( Mg2SiO8 Al(OH)3 ) Ⅰ Antacids NaHCO3+HCl → Nacl+H2O+CO2↑ Mg2Si3O8+4HCl → 2MgCl2+3SiO2 Al(OH)3+3HCl → AlCl3+3H2O Mg(OH)2+HCl → MgCl2+2H2O CaCO3+2HCl → CaCl2+H2O+CO2 ↑ MgO+HCl → MgCl2+H2O 表1、常用抗酸药的作用特点比较 特点 作用 药物 1g药中和0.1 N的HCl ml数 抗酸作用 作用持续时间 保护溃疡面 收敛作用 产生CO2 (嗳气) 引起便秘 引起腹泻 引起碱血症 NaHCO3 Mg2SiO8 Al(OH)3 Mg(OH)2 CaCO3 MgO 120 150 弱快 短 无 无 有 弱慢 长 有 无 无 无 无 有 无 有 无 250 较强慢 较长 有 有 无 有 无 无 210 200 500 较强快 较长 无 无 无 较强快 较长 无 有 有 最强 较长 无 无 无 无 有 无 有 无 无 无 有 无 side reactions: disorder of gastrointestinal track diarrhea; constipation; belching (打嗝); flatulence (肠胃胀气); alkalemia Ⅱ Agents reducing secretion of gastric acid Regulation of gastric acid secretion Proglumide • Drugs reducing secretion of gastric acid (1) H2-receptor antagonists (2) Antimuscarinic agents (3) Inhibitors of the proton pump (4) gastrin-receptor antagonists H2-R antagonists Cimetidine, Ranitidine, Famotidine , Nizatidine [Actions] Competitively block the binding of histamine to H2 receptor. Completely inhibit gastric acid secretion induced by histamine. characteristics: more effective than M-R antagonists;long duration; high rate of healing up; rebound Regulation of gastric acid secretion Proglumide Cimetidine(西咪替丁;甲氰咪胍): [ Pharmacokinetics] • Absorption: p.o F=70% • Distribution: widely • Elimination: kidney • ! Heptic microsomal enzyme inhibitor [ Action] • inhibit all kinds of gastric acid secretion [Clinical uses] ①peptic ulcers : • effective in promoting healing of peptic ulcers. 400 mg bid 4W→80% healing • after treatment is stopped, recurrence is common. This can be effectively prevented by eradication of H.Pylori. • ②Zollinger-Ellison syndrome : a fatal disorder in which a gastrin-producing tumor causes hypersecretion of gastric acid. • In many patients, H2 receptor antagonists can effectively keep the acid secretion to safe levels so as to control symptoms related to excess acid secretion. • ③gastroesophageal reflux disorder (GERD, heartburn): Because they act through stopping acid secretion, they may not relieve symptoms of heartburn for at least 45 minutes. Antacid will be more efficiently to neutralize secreted acid already in the stomach. [Adverse reactions] 1.the common side effects are headache, dizziness, diarrhea and muscular pain, skin rash 2.CNS effects: confusion, disorientation and hallucination 3. Endocrine system effects: gynecomastia, impotency, galactorrhea(溢乳) • Ranitidine(雷尼替丁) • 1) Antisecretive effect is 10 times that of Cimetidine . • 2)Less effect on hepatic microsomal metabolism system. • 3)Longer duration and less antiandrogenic effect • Famotidine(法莫替丁) • 1) Antisecretive effect is 40 times that of Cimetidine . 2) Have no effect on hepatic microsomal metabolism system. • Nizatidine(尼扎替丁): • Ebrotidine(乙溴替丁): 1) ↑Expression of EGF and PDGF→stimulate proliferation of epithelium 2) increase mucus secretion Inhibitors of the proton pump Omeprazole, lansoprazole, pantoprazole [pharmacological effects] • Inhibits H+ being transported to gastric lumen through inhibiting the proton pump. • Potent and long-lasting effect: Can inhibit over 95% of gastric acid secretion. • Also inhibit release of peptin and H.P Regulation of gastric acid secretion Proglumide [Clinical uses] ①peptic ulcer: was judged to be superior to H2-R antagonists ②Zollinger-Ellison syndrome: ③ heartburn : the most effective agents. ④hemorrhage of upper digestive tract ⑤ H.P infection [Adverse reactions] extremely safe • 1)G.I reactions: nausea,vomitting, diarrhea, abdominal pain etc. • 2)NS: headache, swirl, insomnia, peripheral neuritis, etc. • 3) overgrowth of bacteria: Increases in gastric bacterial concentrations. • 4)hypergastrinemia(高胃泌素血症) • 5)canceration Omeprazole • Easily absorbed, but affected by food • Is also heptic enzyme inhibitor lansoprazole second generation Pantoprazole and rabeprazole third generation weak effect on heptic enzyme Antimuscarinic agents • Muscarinic receptor stimulation increase gastrointestinal motility and secretion. • So cholinergic antagonists can be used as adjuncts in the management of peptic ulcer disease and Zollinger-Ellison syndrome, particularly in patients refractory to standard therapies. Regulation of gastric acid secretion Proglumide Antimuscarinic agents • In contrast to the classic anticholinergics, the relatively specific M1-receptor antagonist, Pirenzepine is a good choice as an anti-secretory agent. Because it suppresses basal and stimulated gastric acid secretion at doses having a minimal effect on other organs (salivary glands, the heart and eye.) gastrin-receptor antagonists: • proglumide(丙谷胺) Ⅲ Agents protecting mucosal barrier (1)Prostaglandins (2)Mucosal protective agents Prostaglandins • prostaglandins E2 and I2, produced by the gastric mucosa, inhibit secretion of gastric acid and stimulate secretion of mucus and bicarbonate (cytoprotective effect) . • A deficiency of prostaglandins is thought to be involved in the pathogenesis of peptic ulcers. Mucosal protective agents • These compounds, known as cytoprotective ones , have several actions that enhance mucosal protection mechanisms, thereby preventing mucosal injury, reducing inflammation and healing existing ulcers. clinical uses: NSAID-induced ulcer adverse reactions: dose-dependent diarrhea, stimulate uterus Misoprostol: a stable analog of PGE2 • (1) inhibits secretion of gastric acid and stimulate secretion of mucus and bicarbonate. • (2) dilate blood vessel of mucous membrane. • (3) currently the only agent approved for prevention of gastric ulcers induced by NSAIDs. • (4)less effective than H2-receptor antagonists for acute treatment of peptic ulcers. • (5)produces uterine contractions and is contraindicated during pregnancy. Mucosal protective agents Sucralfate(硫糖铝) 1)In water or acidic solutions it forms a viscous, tenacious paste that binds selectively to ulcers or erosions for up to 6 hours. 2)Also stimulates prostaglandin release and mucus and bicarbonate output. 3)Promote effects of growth factors 4)Inhibit H.P ! Needs acid envioment; affects absorption of other drugs Mucosal protective agents colloidal bismuth subcitrate (枸橼酸铋钾) • 1) binds to an ulcer crater, coating it and protecting it from acid and pepsin. • 2) Inhibits the activity of pepsin • 3) increases mucous secretion • 4) increase prostaglandin synthesis • 5) helps to eradicate H. pylori Antimicrobial agents Optimal therapy of patients with peptic ulcer disease who are infected with H.Pylori requires antimicrobial treatment. Eradication of H.Pylori results in rapid healing of active peptic ulcers and low recurrence rates. Metronidazole, tetracycline, amoxiciliin, etc. Often combined with other drugs. Section 2 Drugs modulating digestive function Ⅰ Digestants Dilute hydrochloric acid Pepsin Pancretin biofermin Ⅱ Antiemetic and prokinetic agents Ⅱ Antiemetic and prokinetic agents ⅰ Antiemetic agents 1. H1-receptor antagonist Dimenhydrinate (乘晕宁) • 2. M-receptor antagonist scopolamine 3. dopamine antagonists: • Metoclopramide(甲氧氯普胺) mechanism 1) block D2-receptor in CTZ → antinausea and antiemetic action 2) block gastrointestinal D2-receptor → promote vermiculation(肠蠕动) • Clinical use: prevention of vomitting gastrointestinal reflux disease nonulcer dyspepsia impaired gastric emptying adverse reaction: extrapyramidal symptoms, especially dystonias(张力障碍) • Domeperidone (多潘立酮) block gastrointestinal D2-receptor → promote vermiculation • Cisapride(西沙必利) DA, Ach, 5-HT • 4. 5-HT3 inhibitor ondansetron : used in the prevention of chemotherapyinduced and postoperative nausea and vomiting Granisetron(格拉司琼) Tropisetron(托烷司琼) Ⅲ Antidiarrheal agents Increased motility of the gastrointestinal tract and decreased absorption of fluid are major factors in diarrhea. So antidiarrheals include anti-motility agents, adsorbents and drugs that modify fluid and salt transport. 1.Opium receptor agonists Opium tincture Tincture camphor compound Diphenoxylate (苯乙哌啶) Loperamide(洛哌丁胺) Diphenoxylate(苯乙哌啶) • Opioids are the most effective agents for relief of diarrhea. • Is an analog of pethidine and have opioidlike actions on the gut. • block gastrointestinal μ-receptor → decrease vermiculation(肠蠕动) • Is used to control acute or chronic functional diarrhea • difficultly penetrate BBB, have no extrapyramidal symptoms 2.Astringents(收敛剂) Tannalbin(鞣酸蛋白) 3.Absorbants Medical charcoal, Smectite(蒙脱石), kaolin , and pectin They act as absorbents of bacteria, toxins, and fluid, thereby decreasing stool liquidity and quantity. They may be useful in acute diarrhea but are seldom used on a chronic basis. Ⅳ Laxatives(泻药) 1.Contact laxatives Phenolphthalein(酚酞), Bisacodyl (比沙可啶) Anthraquinones(蒽醌): rhubarb(大 黄).senna(番泻叶) 2.Osmotic laxatives Magnesium sulfate • Machanism form gels in the large intestine, causing water retention and intestinal distension, thereby increasing motility. • Effects and uses: (1)Diarrhea (2) Cholagogic(利胆的) action (3) Relax skeletal muscles (4)Relax vascular smooth muscle Sodium sulfate, Lactulose(乳果 糖), Glycerol (甘油), castor oil(蓖 麻油) , celluloses(纤维素) 3. Stool softeners Liquid paraffin(石蜡) Ⅴ Choleretics (learn by yourself)