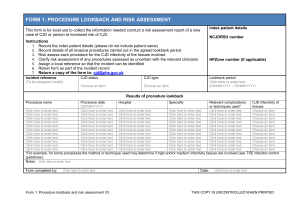
Case Study 78
advertisement

Rapid dementia Richard Lukose PGY-3 Neurology • 54 y/o male accountant presents to PCP • 2 months progressively “acting strangely” per wife – Cannot remember where he parked his car – No longer interested in fantasy football games – Difficulty completing routine tasks at work – Two falls at work while walking in hallway – Grandfather and grandmother with Alzheimer’s Disease onset in their 80’s Physical Exam • • • • • • • • Vitals: 36.8, 18, 84, 132/82 General: NAD, afebrile Head: atraumatic Neck: no nuchal ridgidity, no bruits Chest: CTA Heart: RRR, no murmurs Abdomen: No masses, BS present Extremities: No C/C/E Neurologic Exam • Mental Status: • Alert, oriented to name only • Poor recall of three objects • Poor insight • Poor judgment • Thoughts fragmented • • • • • • CN’s intact Motor 5/5 throughout Reflexes ¾ b/l patellar, toes extensor Sensation: intact for pin/temp/vib/propioception, startle myoclonus Cerebellar: mild b/l ataxia on finger to nose and heel to shin Gait: ataxic with positive Rhomberg test Give a one sentence summary of case Summary • A 54 y/o male without significant medical history with a rapid progression of cognitive decline Summary • A 54 y/o male without significant medical history with a rapid progression of cognitive decline • Neurological exam shows impaired mental status, generalized ataxia, upper motor neuron signs and myoclonus • Mental status change, generalized ataxia, upper motor neuron signs • Localization to the bilateral cerebral and cerebellar hemispheres • Time course? – Rapid! Rapidly Progressive Dementia Differential Diagnosis • VITAMINS: – Vascular: multi-infarct, CNS vasculitis, intravascular lymphoma – Infectious: Encephalitis (bacterial, viral, fungal, rickettsial); Infectious in older adults (UTI, PNA); Progressive multifocal leukoencephalopathy (PML), HIV dementia, Creutzfeldt-Jakob disease; – Toxic/Metabolic: heavy metals, bismuth, drug rxn, electrolytes, Wilson’s disease, vitamin deficiencies, uremic/hepatic encephalopathy Rapidly Progressive Dementia Differential Diagnosis • Autoimmune: CNS vasculitis, Hashimoto encephalopathy, sarcoid • Metastasis (neoplasm): lymphoma, paraneoplastic, primary tumor • Iatrogenic: medications, hospitalization • Neurodegenerative: CJD, Alzheimer disease, obstructive hydrocephalus • Systemic: delirium, hypertensive encephalopathy, mitochondrial Workup: blood tests Geschwind, 2010. RPD: Prion diseases and other RPDs. Continuum 16 (2) 31-56. Required • • • • • • • • • • • • CBC BMP w/ Ca, Mg, Phosphorus LFTs RPR ESR, CRP, antinuclear antibody TSH and free T4 Antithyroglobulin and antithyroperoxidase antibodies B12 HIV Lyme titer Paraneoplastic antibodies Autoimmune antibodies • • • • • • • • Sometimes Helpful Cancer screen Blood smear Coagulation profile Hypercoagulability testing Homocysteine Copper and ceruloplasmin Methylmalonic acid Additional rheumatologic tests Workup: Urine Geschwind, 2010. RPD: Prion diseases and other RPDs. Continuum 16 (2) 31-56. Required • Urine analysis Sometimes Helpful • Urine culture • Copper (24 hrs if Wilson disease suspected) • Heavy metal screen (24 hrs) Workup: CSF Geschwind, 2010. RPD: Prion diseases and other RPDs. Continuum 16 (2) 31-56. • • • • • Required Cell count and differential Glucose IgG index Oligoclonal bands VDRL • • • • • • • • • Sometimes Helpful Cryptococcal antigen Viral PCRs and cultures Vacterial, fungal, acid-fast bacilli stains and cultures Cytology Flow cytometry Whipple PCR 14-3-3 test Total tau Neuron-specific enolase Workup: Other tests Geschwind, 2010. RPD: Prion diseases and other RPDs. Continuum 16 (2) 31-56. Required • MRI brain (FLAIR and DWI) with and without contrast • EEG • • • • • • • • • Sometimes Helpful CT head CT chest, abdomen, pelvis with and without contrast MR angiography brain and neck Mammogram Body PET scan MR spectroscopy Echocardiogram EMG/NCS Brain biopsy Significant Results • CSF – Negative for 14-3-3 protein – Negative for Neuron-specific enolase – Positive for Total Tau EEG: GPEDs MRI: basal ganglia/cortical ribbon on FLAIR WHAT’s YOUR DIAGNOSIS? Sensitivity and Specificity of CSF Biomarkers in UCSF Rapidly Progressive Dementia Cohort from Geschwind, 2010. RPD: Prion diseases and other RPDs. Continuum 16 (2) 31-56. 14-3-3 sCJD = 218 RPD = 90 Neuron-specific enolase sCJD = 86 RPD = 58 Total Tau sCJD = 61 RPD = 35 Sensitivity 55% 57% 64% Specificity 74% 89% 95% sCJD = sporadic Creutzfeldt-Jakob disease; RPD = nonprion rapidly progressive dementia Neuron-specific enolase is considered positive if level is > 35 ng/ml Total Tau is considered positive if level is > 1200 pg/ml False positive rate (FPR) is defined as 1 minus the specificity. FPR 14-3-3 is 26%; NSE is 11% and Total Tau is 5% Creutzfeldt-Jakob Disease • Caused by the transformation of a normal cellular prion protien (PrPc) into a disease causing prion (PrPSc) • Accumulation of PrPSc leads to neurodegeneration 3 CJD Subtypes • Sporadic CJD (sCJD) – 85% of CJD cases – No known cause – Survival 4-8 months – 90% mortality at 1 year – Onset 55-75 years (median age 68, mean 61) – Include sporadic fatal insomnia (very rare) 3 CJD Subtypes • Genetic CJD (gCJD) – Include: familial CJD, Gerstmass-StrausslerScheinker syndrome and fatal familial insomnia – Mutation makes PrP more susceptible to change to PrPSc Familial CJD presents exactly like sCJD 60% of genetic CJD cases have no family history 3 CJD Subtypes • Variant Creutzfeldt-Jakob disease (vCJD) • Bovine Spongiform Encephalopathy (BSE) has been strongly linked to the occurrence of vCJD in humans. • 175 cases in UK and Ireland from October 1996 to March 2011; 3 cases in US. • Containment of the BSE epidemic in cattle resulted in decline of cases of vCJD Criteria for Probably Sporadic CJD WHO revised 1998 • Progressive dementia with any two of: – – – – Myoclonus Pyramidal/extrapyramidal Visual/cerebellar Akinetic mutism – AND typical EEG or if < 2 year duration, positive CSF 14-3-3 AND no other condition to explain USCF Modified (2007) • Rapid cognitive decline with any two of: – – – – – – Myoclonus Pyramidal/extrapyramidal Visual Cerebellar Akinetic mutism Other focal higher cortical sign – AND typical MRI and/or EEG – AND no other condition to explain CJD MRI findings now thought to be best test for CJD sCJD and gCJD – cortical riboning and basal ganglia involvement on DWI vCJD – Pulvinar sign on DWI and FLAIR is said to be 90% sensitive for vCJD Definitive diagnosis of CJD can only be made through autopsy • spongiform change in the gray matter • the presence of many round vacuoles in all six cortical layers or cortex or with diffuse involvement of the cerebellar molecular layer • vacuoles appear glassy or eosinophilic and may coalesce • Neuronal loss and gliosis are also seen • Plaques of amyloid-like material can be seen in the neocortex in new-variant CJD. CJD Links • Autopsy H&E • Biopsy H&E