Slide 2 - On The CUSP
advertisement

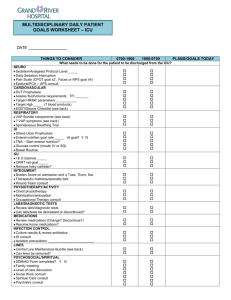
CLABSI Supplemental Call Series Ventilator Associated Pneumonia Prevention Sean Berenholtz, MD MHS FCCM September 20, 2011 at 2ET/1 CT/12 MT/11 PT Your Feedback is Important https://www.surveymonkey.com/s/Z6FJ28T Slide 2 Learning Objectives •To describe the morbidity and mortality associated with Ventilator Associated Pneumonia •To understand the framework used to achieve substantial and sustained reductions in VAP as part of the Michigan Keystone ICU program •To outline next steps towards implementing VAP prevention efforts Slide 3 Impact of VAP • 10-20% of ventilated patients • Common HAI – Median rate 1-4.3 per 1000 vent day – 250,000 infections per year • Most lethal HAI – Mortality likely exceeds 10% – Up to 36,000 deaths per year • Cost per episode: $23,000 Safdar CCM 2005, Kollef Chest 2005, Perencevich ICHE 2007, Public Health Rep. 2007. Slide 4 Healthcare Associated Pneumonia Prevention • CDC/HICPAC: Guidelines for the Prevention of Healthcare Associated Pneumonia; 2004. • Canadian Critical Care Trials Group1: Comprehensive evidence-based clinical practice guidelines for ventilatorassociated pneumonia: Prevention. Journal of Critical Care; 2008. • SHEA/IDSA: Strategies to Prevent Ventilator-Associated Pneumonia in Acute Care Hospitals; 2008. Slide 5 How Can These Errors Happen? • People are fallible • Medicine is still treated as an art, not science • Need to view the delivery of healthcare as a science • Need systems that catch mistakes before they reach the patient Slide 6 To Improve Reliability • Standardize what is done, when it is done – Reduce complexity • Create independent checks for key processes – How often do we do what we should • Learn from defects – How often do we learn from defects Health Services Research 2006; Circulation 2009;119:330-337. Slide 7 Improving Care for Ventilated Patients • Semirecumbant positioning • Peptic ulcer disease and DVT prophylaxis • Appropriate sedation • Daily assessment of readiness to extubate • Oral care with antiseptics • Minimize contamination of equipment Slide 8 Translating Evidence into Practice Pronovost, Berenholtz, Needham. BMJ 2008 Slide 9 Improving Care for Ventilated Patients • Engage – Partner with infection preventionists, – Post performance, – Tell stories of harm • Educate – Reviewed evidence on conference calls, – One-page fact sheets, – Slides for teams Slide 10 Improving Care for Ventilated Patients • Decrease complexity / create redundancy – Standardized order sets and protocols – Daily goals checklist • Other independent redundancies – Nursing and families – Are patients receiving the prevention they should? Slide 11 Sample Daily Goals J Crit Care 2003;18(2):71-75 Slide 12 Improving Care for Ventilated Patients Evaluate • VAP – Standardized CDC NHSN definitions for VAP – VAP definition varies; Did not change definition • Ventilator Bundle Process Measures – – – – Collected by the ICU teams; daily cross-sectional sample Standardized definitions and data collection forms Limited number of trained data collectors After first quarter of daily data collection, teams were allowed to collect process measures one to two days/week (min of 15 vent pts/mo) to minimize burden. Slide 13 Results • 124 of 127 ICUs submitted VAP data – 12 ICUs started after funding ended • 112 ICUs, 72 hospitals included in analysis • 3228 ICU months and 550,800 vent days • 10% quarters without complete data – 4% missing data; 6% stopped submitting data • Sensitivity analysis yielded similar results • Results reported through 28-30 months postimplementation Slide 14 Michigan Keystone ICU % Percent of ventilator days where patients received all five therapies Quarterly Composite Ventilator Bundle Adherence Over Time 100 80 60 40 20 0 Time (Months) Infect Control Hosp Epidemiol. 2011;32(4):305-314. Slide 15 Michigan Keystone ICU (n= Infect Control Hosp Epidemiol. 2011;32(4):305-314. Slide 16 Limitations • Lack of concurrent control group – Temporal changes, other interventions • Did not evaluate accuracy of VAP diagnosis – All hospitals reported using CDC definitions – Used existing hospital infrastructure • Can not evaluate importance of individual therapies in ventilator bundle • Can not evaluate importance of other intervention • Focus on ventilator care vs VAP prevention Slide 17 Strengths • • • • Largest cohort to date Significant and sustained VAP reductions Focus on system of care Engagement of local interdisciplinary teams to assume ownership • Centralized support for technical work • Local adaptation of intervention • Culture improvement and social networking among ICUs Slide 18 Summary • VAP is most lethal HAI; majority are preventable • Effective interventions to prevent VAP are known; patients are not receiving the care they should • Focus on systems to ensure patients receive the therapies they ought to Slide 19 Next Steps • Keystone ICU VAP project focused on ‘Ventilator Bundle’ • Developing ‘VAP prevention bundle’ – Funded by NIH/NHLBI – Delphi process led by RAND researcher Slide 20 European Care Bundle for VAP Prevention Intensive Care Med 2010;36:773-780 Slide 21 Your Feedback is Important https://www.surveymonkey.com/s/Z6FJ28T Slide 22