Imaging in headache patients
advertisement

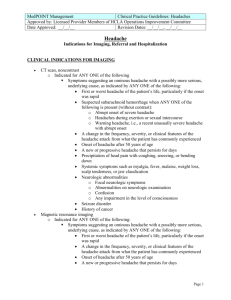
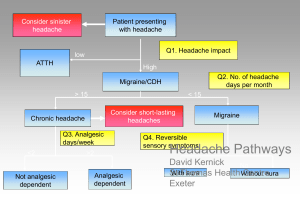
Imaging in headache patients “Incidentalomas” Giles Elrington Barts & The London elrington@aol.com To scan or not to scan Scan everyone • Safe? • Reassuring? Selective scanning • How selective? Scan no-one • Not recommended! Where is the disease? SYMPTOMS ABNORMAL TESTS PATHOLOGY BASH guidelines 2007 “Investigations, including neuroimaging, do not contribute to the diagnosis of migraine or tensiontype headache. Some experts, but not all, request brain MRI in patients newly diagnosed with cluster headache. There are no data on the rate of abnormal findings. Otherwise, investigations are indicated only when history or examination suggest headache is secondary to some other condition.” IHS classification 2004 Primary headache… • Is not attributed to another cause; i.e. • History and physical examination do not suggest any of the disorders listed in groups 5-12 (i.e. secondary headache), or history and/or physical and/or neurological examinations do suggest such disorder but it is ruled out by appropriate investigations, or such disorder is present but attacks do not occur in close temporal relationship to the disorder Demography of headache • • • • 95% have headache in their lifetime 75% have headache in any year 20% of women have migraine 4% have headache on most days Serious cause for headache • Primary care • Neurology clinic • Accident & emergency 0.1% 1% 10% Three cases All normal to examine • Male 80. 3/12 R facial pain. Longstanding headache. • Female 47. 30 yr episodic headache better off COC, worse 4yr, continuous 1yr. • Female 74. Few months right craniofacial pain, partial response NSAID. Unenhanced CT overlooks important secondary headaches • • • • • • • • • • Early tumours Early stroke Giant cell arteritis Venous sinus thrombosis Subarachnoid haemorrhage Subdural haematoma Tonsillar ectopia Colloid cyst Parameningeal suppuration Medication overuse headache Imaging urgent: red flags tumour risk>1% • Papilloedema • Significant change consciousness, memory, confusion, coordination • New epileptic seizure • New cluster headache • Cancer elsewhere Imaging low threshold: orange flags tumour risk 0.1-1% • • • • • • • New headache undiagnosed >8weeks Significant neurological findings Headache worse exertion/Valsalva Headache with vomiting Changed or crescendo headache New headache pt over 50 yrs Headache waking from sleep Imaging yellow flags tumour risk 0.01-0.1% • • • • Migraine or TTH Weakness or motor loss Memory loss Personality change Incidentalomas • Age 20 – n= 2389 – ¼ not strictly normal – ¾ of these = normal variants • Age 45-97 – n=2000 – ⅛ significant abnormality One of these six has no headache…which one is it? MRI result may be harmful... • • • • Female age 38 Migraine with aura Medication overuse MRI arranged in primary care Two recent cases… Headache imaging 1994-2001 (n=2488) 60 50 % 40 MR & CT 30 MR CT 20 10 0 1 2 3 4 5 Year 6 7 8 Headache imaging 1994-2008 (n=4971) 60 50 % 40 %CT & MRI 30 % MRI %CT 20 10 0 1992 1994 1996 1998 2000 2002 Year 2004 2006 2008 2010 Incidentalomas Morris et al BMJ 2009;339:547-550 • • Systematic review and meta-analysis of MRI brain scans of 19,559 ‘normal’ subjects Neoplastic, structural vascular, inflammatory lesions, cysts, other structural lesions. Excluded: ‘white matter hyperintensities’, silent infarcts, microbleeds Lesion Prevalence % ‘NNS’ Neoplasms Meningioma 0.29 (0.13-0.51) 345 Pit. Adenoma 0.15 (0.09-0.22) 667 Low grade glioma 0.05 (0.02-0.09) 2000 TOTAL 0.7 (0.47-0.98) 143 Other 2.0 (1.13-3.10) 50 TOTAL 2.7 37 Imaging for headache • A&E: – low threshold – CT > MRI – Don’t forget LP, ESR(CRP) • Office practice: – higher threshold – MRI > CT Imaging for all • Covers your back • Improves provider income • May temporarily reduce most patients’ anxiety • Emotion based • Expensive • Scan only as good as the report • Longer waits disadvantage those in urgent need • Creates precedent • Diminishes non-imaged diagnoses • Causes harm to minority Selective imaging • Evidence based • Economical • Places clinical diagnosis first • Allows prioritisation • Incomplete precision • Litigation risk • Reduces provider income Headache imaging: conclusions • • • • Suggest selective imaging policy Acute presentation: CT (NB LP, ESR) Non-acute: MRI First scan: – Patient (emotion) led • Subsequent scan: – Doctor (evidence) led