10. Tüdõtuberculosis, Mycobacteriosis
advertisement

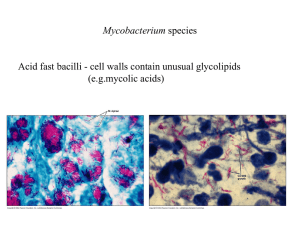
Tuberculosis Bálint Beatrix MD, PhD SZTE, Dpt. of Pulmonology Deszk 2014. Tuberculosis TB a chronic bacterial infection, causes more deaths worldwide than any other infectious disease. TB is spread through the air and usually infects the lungs, although other organs are sometimes involved. Some 2 billion people - one-third of the world's population - are infected with the TB organism, Mycobacterium tuberculosis. History 1. Paleopathological evidences - skeletal TB, bone TB Ancient greek physisians used the word PHTYSIS 8th-9th century ¼ of the european adults died from TB. Germ theory: -Robert Koch (1882)-Pathogenicity of Mycobacterium tuberculosis -Konrad Röntgen (1892)- X ray TB in the World (number of TB cases) Románia Oroszország Portugália Szerbia Lengyelország Magyarország 2005 Spanyolország Szlovénia 2004 Nagy-Britannia 2003 Szlovákia 2002 Ausztria Belgium 2001 Csehország Franciaország Németország Hollandia Finnország Olaszország Dánia Svédország % 000 Tbc incidencia Európában az elmúlt években TB in EUROPE 2006 160,0 140,0 120,0 100,0 80,0 60,0 40,0 20,0 0,0 Causes of death of HIV positive patients Mycobacterium tuberculosis • • • • The causative agents for tuberculosis Discovered by Robert Koch in 1882 ~25 % of world’s population infected 25 million is infected in USA Microbiology Mycobacterium tuberculosis obligate, aerobic parazite, acid-fast slow growth visible colonial growth: 4-6 weeks INH resistant and sensitive strains are different Direct examination Ziehl-Neelsen stain: 4 m long and 0,2-0,5 m wide 10 000 organism/ml of sputumsmear positive Culture of sputum/fluid M. tuberculosis: growths slowly, lack of pigment, produces niacin M. bovis: niacine negative Drug sensitivity test. Quick test: PCR, Bactec Mode of spread • TB is spread from in microscopic droplets person to person — droplet nuclei — expelled from the lungs when a TB sufferer coughs, sneezes, speaks, sings, or laughs. Only people with active disease are contagious. • People are most likely to be contagious when their sputum contains bacilli, when they cough frequently and when the extent of their lung disease, as revealed by a chest x-ray, is great. * People who have been treated with appropriate drugs for at least two weeks usually are not infectious. Predisposing Factors • • • • • • • • • • Babies and young children HIV infection substance abuse diabetes mellitus silicosis cancer leukemia or Hodgkin's disease severe kidney disease low body weight certain medical treatments – corticosteroid treatment – organ transplants – chemotherapy HOW DOES TB DISEASE DEVELOP? There are two possible ways a person can become sick with TB disease: 1.A person who may have been infected with TB for years and has been perfectly healthy. The time may come when this person suffers a change in health. The cause may be another disease like AIDS or diabetes. Or it may be drug or alcohol abuse or a lack of health care because of homelessness. Whatever the cause, when the body's ability to protect itself is damaged, the TB infection can become TB disease. In this way, a person may become sick with TB disease months or even years after they first breathed in the TB germs. 2. A person first breathes in the TB germs the body is unable to protect itself against the disease. The germs then develop into active TB disease within weeks. (This way TB disease develops happens much more quickly.) Pathogenesis The site of initial infection alveoli macrophages ingest the inhaled M. tuberculosis. Some bacilli may be killed immediately; others may multiply within the macrophages. During the 2 to 8 weeks after initial infection in people with intact immune systems, macrophages present pieces of the bacilli, displayed on their cell surfaces, to the T cells release an elaborate array of chemical signals cell-mediated hypersensitivity T cells responds tuberculin skin test (PPD test) cell signals inflammatory reactions; recruit and activate specialized cells to kill bacilli and In HIV-infected people and in children, the bacilli spread to other sites in the body dissemination life-threatening meningitis and other problems. Pathogenesis 2. The body's immune system maintains a standoff with the infection, sometimes for years. TB bacilli may persist within macrophages, but further multiplication and spread of M. tuberculosis are confined. Most people undergo complete healing of their initial infection, and the tubercles calcify and lose their viability. A positive TB skin test, and in some cases a chest x-ray, may provide the only evidence of the infection. If, the body's resistance is because of aging, infections (HIV), malnutrition,or other factors, the bacilli may break out of the tubercles in the alveoli and cause active disease. Pathogenesis 3. (X ray) Simon foci: The initial infection leaves nodular scars in the apices of one or both lungs, called which are the most common seeds for later active TB. Ghon foci: calcified scars of primary infection and residual calcified hilar lymph nodes. Ghon komplex Symptoms Early TB (single or multiple nodule, caseous lesion) - no symptomes Progresszive TB (cavitation, pneumonitis) - nonspecific symptomes: anorexia, fatigue, weight loss, remittent fever, night sweets - cough, sputum (mucopurulent) - haemoptysis - chest pain (inflammation of parietal pleura) Laboratory findings IIn advanced TB! - RBC - Se albumin - WBC - Sodium - Calcium Characteristic X-ray findings • • • • Apical, subapical patchy infiltration Bilateral upper lobe infiltration Dissemination: miliary tb Lower lobe TB – cavitation or infiltration – atelectesis, mass leasions, large cavitation with fluid, pneumonic-like infiltration • Non-specific • Pleural effusion Tbc: tuberculoma Tb pneumonia Tb hilar adenopathy Miliary tb Tb: miliary Tb: cavity Tb: cavity Tb: cavity Tb:progressive Callus pleurae, residuum Diagnosis • X-ray findings • Sputum/bronchoscopic lavage fluid smear + Negatíve tuberculin test: can not exclude the infection • Histology: TUBERCULOMA • epitheloid cells, •Langhans giant cells, •lymphocytes, •caseous lesion (necrosis) •Definitive diagnosis - culture - specification of the organism Extrapulmonary TB (TB can involve any organ) -TB of the tonsils, lymph nodes, abdominal organs, bones, and joints caused by ingestion of milk infected with M. bovis. (slaughtering cows with milk) *GENITOURINARY TUBERCULOSIS -kidney pyelonephritis. (chronic, "sterile" routine culture-negative) -epididymis or prostate gland, baldder, vesicles. -Salpingo-oophoritis * TUBERCULOUS MENINGITIS (TB to the subarachnoid space) * MILIARY TUBERCULOSIS (Generalized Hematogenous or Lymphohematogenous TB) Bone marrow involvement * TUBERCULOUS PERITONITIS *TUBERCULOUS PERICARDITIS *TUBERCULOUS LYMPHADENITIS *TUBERCULOSIS OF BONES AND JOINTS (Pott's disease) *TUBERCULOSIS OF THE LIVER Extrapulmonary TB according to the location (Hungary 2007.) Extrapulmonalis tuberculosis lokalizáció szerint Pleuritis és egyéb 48% Csont-izületi 13% Nyirokcsomó 13% Meningitis 3% Hugy-ivarszervi 16% History of chemotherapy Streptomycin Toxicity Resistancy Recidive infection 1946-1952 Isonicid 1952-1970 INH + PAS + Streptomycin Treatment-18 months Rifampicin RMP + INH RMP + INH + ETB 1970 9 months 6 months Therapeutic agents for tb • • • • • • First line therapy Isoniazid Rifampin Pyrazinamide Streptomycin Ethambutol • • • • • • Secund line therapy Ethionamide Cycloserine PAS Aminoglycosides Capreomycin Activity of antituberculous drug Drug Activity pH Site Isoniazid Rifampin Pirazynamide Ethambutol cidal cidal/static cidal/sterilizing cidal at 25 mg/kg static at 15 mg/kg cidal neut-alk neut-alk acid neut-alk I/E I/E I/E I/E neut-alk E Streotomycin I=Intracellular; E=Extracellular Second line drugs • • • • • • • Aminoglycosides Capreomycin Ethionamide PAS Cycloserine Ciprofloxacin Ofloxacin • • • • Thiocetazone Imipenem Ampicillin Metronidazole Characteristics of 2nd line drugs • • • • • Less effective drugs Poor GI tolarence Significant side effect profile Not well studied Some not readily available (PAS) The principles of therapy • Combination therapy – kills more effectively – Shortens therapy • Prevents emergence of resistance: – INH/RAMP EMB SM PZA • • • • Treatment must be for a least six month Bactericidal phase: 1 month Strerilizing phase: months 3 through 6 Never add a single drug t a failing regimen Initial therapy: four drugs • • • • Isoniazid (INH) 300 mg daily Rifampin (RIF) 600 mg daily Pyrazinamide (PZA)25-30 mg daily Ethambutol (EMB)25 mg initially Therapeutic Regimens • • • • • Daily therapy 6 months Daily treatment 180 doses 2-3 % relapse • Short course • 6 months • Twice or three times weekly • 52-114 doses • Equivalent relapse Preventive therapy for tuberculous infection • Infection vs. active disease • Lifetime risk for active disease – Higher in children – 10 % per year in HIV infected patients • Mantoux skin test is the indicator of infection • Preventive therapy requires 6 months of single drug therapy • Isoniazid Nontuberculous mycobacteria • Pumonary disease – M. avium, kansasii, abscessus, xenopi, malmoense • Lymphadenitis – M. avium, scrofulaceum, malmoense • Cutaneous disease – M. marinum, fortuitum, chelonea, ulcerans • Disseminated disease – M. avium, kansasii,chelonea, haemophilum Treatment of nontuberculous mycobacteria • The antituberculotic drugs are usually not effective • M. kansasii: INH, RIF, EMB • M. avium: macrolide, Rifamycin, EMB • Rapid growers: clarithromycin and 2nd agents History 2. Outstanding representatives of the arts and political life who suffered from TB • • • • • • • • Balzac Brontë sisters Chekov Chopin Dostoevsky Kafka D.H. Lawrence Sir Walter Scott • • • • E. A. Poe Voltaire John Keats Rembrandt’s wife (Sashka) and his son (Titus) • Marquise de Pompadur • Napoleon II Model: Simonetta Catanea died of TB at the age of 23. Symptomes:whitish-pink colour of skin, small shoulders, narrow thorax, low-placed and close breastssigns of phtisis